
Hot Stuff Bias and Diagnostic Drift
One of the problems caused by a disease going hot is hot stuff bias. This is simply human nature at work. If everyone is talking about covid, then every respiratory patient starts to look like a covid patient. Add in a covid test that is so sensitive it can detect viral dandruff left behind from past infections, and the conditions are right for a form of diagnostic drift, which happens when a diagnosis accumulates patients that don’t properly belong to it. Is there any evidence this might be happening with covid?
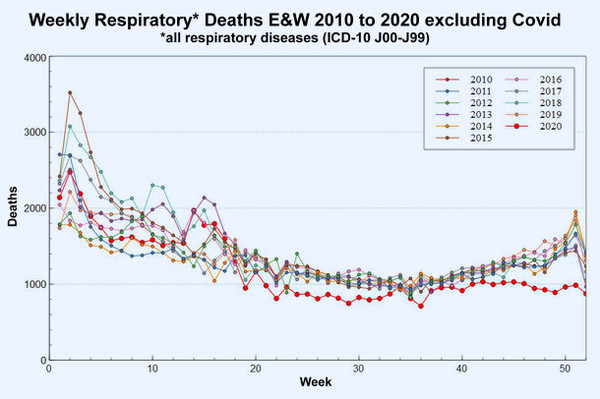
The answer is yes, even if there is another plausible explanation, which Dr No will come to shortly. ONS have reported weekly deaths for England and Wales from all pre-covid respiratory deaths for the last decade, and the image for this post charts them for each year. Note that these are all respiratory deaths, but a good many — perhaps one third to getting on for half or more in a bad flu year in winter — will be influenza and pneumonia deaths — see footnotes for some background details. What we see is that for every year apart from 2020, the pattern is similar and familiar. Putting aside the year start/end effects caused by incomplete weeks, the first 20 weeks of the year are ravaged by flu, then things settle down over the summer, only for mortality to rise as autumn and then winter arrive.
But if we look at the 2020 line, red and a bit heavier than the other lines, something different happens. Up until week 20, it is lost in the general noise, but over the summer it is a little bit below normal, and then, come the autumn, the normal and expected upturn does not appear. Respiratory deaths continue to flat line, and then show a very unexpected fall from about week 47. Very recent weeks may have incomplete data, but most of that fall is likely to be real.
There are two plausible explanations. The first is hot stuff bias and associated diagnostic drift. Patients dying from influenza and pneumonia are incorrectly being classified as covid deaths, perhaps based on clinical suspicion fuelled by hot stuff bias, or by a loosening of diagnostic criteria, for instance, by finding some historical viral dandruff, without properly considering the clinical picture. Given that there are, by mid December, some 500 or so ‘missing’ weekly respiratory deaths, with many of them likely to be ‘missing’ excess winter flu and pneumonia deaths, it is entirely possible these normal winter 2020 excess non-covid deaths have been incorrectly given a covid cause of death, so inflating covid deaths.
The other plausible explanation is that they are indeed all or mostly covid deaths. What has happened is that covid, for want of a better phrase, has grabbed a number of patients who would in pre-covid years have been influenza and pneumonia deaths, but have in 2020 become covid deaths. These deaths, though from covid, are part of the normal winter excess deaths, and not excess covid deaths. They are part of a normal pattern, who just happened to succumb to covid, rather than another respiratory infection.
We can speculate until we are blue in the face — perhaps a rather too apposite turn of phrase, given these are respiratory deaths — about what happened to those desaparecidos respiratory deaths in late 2020. Some will even suggest they weren’t true desaparecidos, they were instead really disappeared, or rather prevented, by anti-covid measures, which worked to reduce all contagious respiratory deaths. But Dr No thinks that is unlikely, partly because he doubts the general effectiveness of the measures, and partly because old frail folk have an awkward habit of dying, and so the 500 or so missing respiratory deaths each week will have turned up somewhere, just not as respiratory deaths. Dr No’s hunch — and Dr No allows himself the occasional hunch — is that both the plausible explanations given above are in play, but by far the bigger effect comes from hot stuff bias and diagnostic drift.
Footnotes
| J00-J06 | Acute upper respiratory infections |
| J09-J18 | Influenza and pneumonia |
| J20-J22 | Other acute lower respiratory infections |
| J30-J39 | Other diseases of upper respiratory tract |
| J40-J47 | Chronic lower respiratory diseases |
| J60-J70 | Lung diseases due to external agents |
| J80-J84 | Other respiratory diseases principally affecting the interstitium |
| J85-J86 | Suppurative and necrotic conditions of the lower respiratory tract |
| J90-J94 | Other diseases of the pleura |
| J95-J95 | Intraoperative and postprocedural complications and disorders... |
| J96-J99 | Other diseases of the respiratory system |
Average numbers of December (so a month, not a week) deaths 2015-2019 for leading ICD-10 Codes J00-J99 respiratory causes of death in England (not E&W), from here:
| Acute respiratory infections other than influenza and pneumonia | 433 |
| Chronic lower respiratory diseases | 2950 |
| Influenza and pneumonia | 2534 (1) |
| Pulmonary oedema and other interstitial pulmonary diseases | 535 |
(1) ~40% of all respiratory deaths; for weeks 48 to 51 in 2020, average weekly respiratory deaths were ~30% less than in the previous ten years
Interesting read, which makes much sense.
Dr No’s conclusions (with some assumptions) all add support to the argument that we have become obsessed with Covid. If we took away the demonised label, which stokes fear and called it Flu / Respiratory Illness, would we notice any real significant difference in our everyday lives? The media’s constructed ‘moral panic’ has ploughed through all moderate thoughts and opinions within our societies.
My argument is that Covid has only become notable because we are obsessing over it. Not that ignorance is bliss, but it would at least calm matters down and help us to gain perspective – to then sensibly look at ‘illness, rather than cases’, ‘actual deaths rather than probability models’ and so on…
‘ …really disappeared, or rather prevented, by anti-covid measures, which worked to reduce all contagious respiratory deaths.’
If anti-CoVid measures worked on other respiratory disease, wouldn’t they work on CoVid too? So wouldn’t there be a big fall in CoVid assigned deaths/cases?
If the measures are working, why do ‘cases’ keep going up requiring more measures?
Infection being a competitive market, displacement by new kid on the block and biased misdiagnosis seem most likely explanation.
Similar situation in other Countries from what I read.
According to EUROMOMO, excess Winter deaths in Sweden within normal range back to 2015; ditto UK; France; Spain – even Italy only marginally more than 2017.
“If the measures are working, why do ‘cases’ keep going up requiring more measures?”
To start with, “cases” as currently used by the NHS, media and government denotes merely a positive test (PCR or lateral flow). There is abundant evidence that such tests are more or less meaningless.
Now if such tests were simultaneously carried out for all the other respiratory diseases listed in the table… that would be interesting. I conjecture that we would seem to have “pandemics” of them, too.
The important questions are: how many people are dying? And how many people are actually sick? Once a person has been diagnosed as sick by a doctor, using conventional diagnostic methods, then it is time to use a PCR test to try and find out what virus is causing the illness.
Very often, medical fashions can cause panics. For example, when someone invented a machine to compute the amount of “cholesterol” in blood, there was an immediate stampede to buy (and, of course, sell) such machines, and to write papers describing how useful they were.
As we now know, “cholesterol” without further qualification is a meaningless measurement. But, as we know, you get what you measure; and, it seems, you measure whatever you can.
RIP, homo insipiens.
I’ve been scratching my head trying to think of any mercies in the present situation.
I’ve come up with one. The Jew-baiters who infest some corners of the internet haven’t invented the word Coyid to summarise the case that it’s all a Jewish conspiracy. In fact I haven’t even seen them try to make that case, presumably because they think it’s all a Chinese conspiracy.
https://www.statista.com/statistics/1178046/influenza-pneumonia-and-covid-19-deaths-in-england-and-wales/