
More or Less Getting It Wrong
Putting a bionic cat among the catatonic pigeons, the much publicised only 17k deaths from covid figure has led to some of the most acrimonious splats Dr No has ever seen on squitter, the social media platform on which participants dump on each other from great heights. Joining the general opprobrium, Tim Harford used the first slot on this week’s More or Less programme on Radio 4 to apply ‘tireless debunkery’ to the claim, with more or less help from a molecular biologist who got her ONS numbers mixed up, claiming (at about 3:12) that the 17k deaths were covid–19 deaths where “no other health condition was mentioned on the death certificate”, which is not true: the actual number of deaths where no other condition was mentioned — that is, deaths where covid–19 was the only cause mentioned — is even smaller, at 6,183. The 17k figure, on the other hand, represents covid–19 deaths with no pre-existing conditions, or as ONS also calls them, deaths from covid-19 with no other underlying causes; but that is not to say there were no other causes mentioned. Other causes may have been present, but they were not deemed by ONS to be pre-existing, or underlying causes.
This matters, because of the way ONS codes the underlying cause of death when covid–19 appears in Part I of the MCCD, or Medical Certificate of Cause of Death. Undeterred, the radio presenter with a voice like audio Horlicks ploughed on: as it is with hand grenades and horseshoes, in the land of tireless More or Less debunkery, near enough is more or less good enough. After some preliminary waffle, the piece then degenerated into a caring and sharing so much it hurts wokist wail about not counting the tens of thousands of alleged additional covid–19 deaths, over and above the 17k deaths, that appear, for example, on the government’s coronavirus dashboard. No one, least of all Dr No, is not counting these deaths. Instead, all he wants to know is where these additional deaths should be counted: in a covid–19 column, or in a non-covid–19 column?
To understand what is going on here, we need to return again to how ONS codes causes of death. The covid–19 coding rules come from WHO, and they place a premium on collecting as many deaths with covid–19 as underlying cause deaths as possible, reflecting not medical veracity, but what WHO airily calls “interests of importance for public health”. The rules are crystal clear that public interests take precedence over medical accuracy: “…whether a sequence [chain of events leading to death, and so underlying cause] is listed as ‘rejected’ or ‘accepted’ may reflect interests of importance for public health rather than what is acceptable from a purely medical point of view. Therefore, always apply these instructions, whether they can be considered medically correct or not (emphasis added).”
These instructions, which apply to a number of infectious and parasitic diseases, are in fact an established pre-covid–19 procedure, embedded in WHO’s ICD–10 Volume 2 Instruction Manual Fifth Edition dated 2016, which has been adopted by ONS, and indeed most other nations. Coders are instructed to reject sequences of events leading to death that place these diseases as due to any other causes (ie they are not the underlying cause): “Do not accept [these] infectious and parasitic diseases as due to any other causes, not even HIV/AIDS, malignant neoplasms or conditions impairing the immune system”. The effect is that these infectious and parasitic diseases almost always (there are a few exceptions, for instance external causes such as trauma) trump any other potentially valid underlying cause of death to become the underlying cause of death, even if it makes no sense from a “purely medical point of view”. All that happened when covid–19 arrived was that these rules were also applied to covid–19.
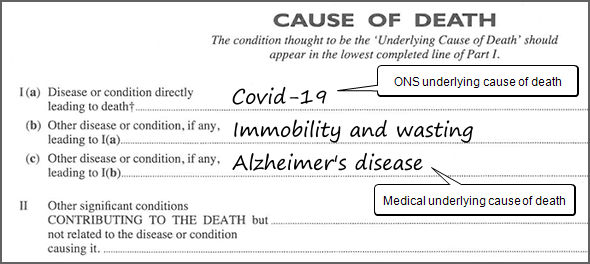
The effect of this rule, as noted, is that the infectious diseases listed, including covid–19, almost always trump other potentially valid underlying causes of death. A sequence of events such as metastatic lung cancer leading to covid–19 infection leading to pneumonia will be coded with covid–19 as the underlying cause, when in non-covid–19 circumstances lung cancer would be the underlying cause. Likewise, the normally accepted sequence Alzheimer’s disease leading to immobility and wasting leading to bronchopneumonia, with Alzheimer’s as underlying cause, would, if covid–19 was present on a higher line — as shown in the image at the top of this post — be coded with covid–19 as the underlying cause, even if it makes no sense from a “purely medical point of view”. We can all no doubt see where WHO, and all the organisations that have adopted WHO’s guidelines, are coming from: an ardent desire to bump up the numbers to grab global and political attention in the face of certain infectious diseases. But at the same time, we should not forget that, by the same token, covid–19 death counts are deliberate collected in a manner intended to “reflect interests of importance for public health…whether medically correct or not”. Or to put it more bluntly: the numbers may be inflated, possibly wildly inflated.
We can now return to the 6,183 deaths, the 17k deaths, and more or less 140k deaths — all the counts cover, give or take a few days, from the start of the pandemic to the end of 2021 — and consider what they really represent. Harford’s stooge may have got her knickers in a twist, but we can straighten them out. The 6,183 deaths are those where COVID-19 was the only cause mentioned. Dr No takes this to mean there was only one entry in Part I of the MCCD (Medical Certificate of Cause Death), and it said covid–19: the underlying cause of death was covid–19, the whole covid, and nothing but the covid. Fair enough: if there is only one entry, then that has — unless it is nonesense — to be the underlying cause of death. But that only covers a tiny fraction, 6,183, of all the deaths. Nonetheless, these 6,183 deaths were true (insofar as the MCCD records the death) covid–19 deaths.
The 17k covid–19 deaths — often this FOI response is often given as the source, but more up to date and detailed routine data that was used for the FOI response can be found here and it includes data to the end of 2021 — are harder to tease out. The count is actually a count of all covid deaths with no pre-existing conditions, which, as we noted earlier, is not the same thing as no other conditions. There may well have been other conditions present in Part I of the MCCD, but, for whatever reason, they were not deemed to be pre-existing, or underlying cause of death, conditions. And herein lies the rub: there is no way of knowing how often in these deaths covid–19 made sense “from a purely medical point of view” — ie covid–19 really was the true underlying cause of death — and how often, under the covid–19 coding rules, covid–19 trumped another perfectly legitimate underlying cause of death that, without covid–19 presence on the MCCD, would undoubtedly be the underlying cause of death. Even worse, exactly the same problem applies to all the other “due to covid–19” deaths, all 140k of them (140k being 175k less 10% as covid–19 was not the underlying cause, even though it was on the MCCD, and then minus the 17k).
Dr No suggests that from a true public health perspective, this ambiguity in the numbers is a epidemiological disaster, which means nothing less than we have no accurate way of knowing the true extent of covid–19 mortality. Is the sequence of events shown in the image at the top of the post — Alzheimer’s disease leading to Immobility and wasting leading to Covid–19 — really a covid–19 death, as ONS would count it, or it really an Alzheimer’s death, with covid–19 being the final consequent event in the sequence of events that lead to death? How many times has covid–19 been allowed to trump an otherwise perfectly valid underlying cause of death, that indeed would have been the cause of death, had covid–19 not appeared on Part I of the MCCD?
Even if they have the data, which Dr No doubts, ONS are hardly likely to tell us how many times covid–19 was allowed to trump another valid underlying cause. Dr No’s favourite statistic, all cause mortality, is of no help on this, because there is no cause of death information in the data, and so, if there are excess deaths, we cannot even know whether they are covid–19 deaths, or covid–19 response deaths, caused by lockdowns, delayed diagnosis and treatment, let alone whether covid–19 trumped other causes. But there is one thing we can look at that might give us a somewhat vague clue — do not for a moment consider it more than that — as to how often covid–19 steals the underlying cause of death from the jaws of other normally common underlying causes of death: the numbers of those deaths from common causes in 2020 and 2021, compared to those in previous years. Our hypothesis, such as it is, is that if covid-19 has trumped deaths from these other causes, then there will less of them in the last two years.
Dr No cannot underline strongly enough that this is a very oblique way of approaching this question. It may be that covid–19 trumping, when it happened, was legitimate: covid–19 really was the underlying cause of death. But then again, maybe not; and as we have no other way of approaching the question, it is at least a way of looking at the data, that might give us cause for thought. With the caveats established, Table 1 shows the average annual numbers of deaths for common causes for 2015-2019, and the numbers in 2020 and 2021. We’ll stick with numbers, which we have covered so far in this post, and which are easier to grasp than the also available but more abstract age standardised rates, though they tell pretty much the same story. The data comes from ONS’s monthly mortality reports, available here.
| Underlying Cause of Death | 2015-2019 | 2020 | 2021 |
| Dementia and Alzheimer's disease | 61,928 | 66,060 | 57,673 |
| Ischaemic heart diseases | 53,429 | 51,979 | 52,821 |
| Cerebrovascular diseases | 29,943 | 27,681 | 27,092 |
| Malignant neoplasm of trachea, bronchus and lung | 28,108 | 26,571 | 26,389 |
| Chronic lower respiratory diseases | 29,681 | 26,917 | 24,319 |
| Symptoms, signs and ill-defined conditions | 12,078 | 14,385 | 15,242 |
| Influenza and pneumonia | 25,969 | 18,656 | 15,148 |
| Malignant neoplasm of colon, sigmoid, rectum and anus | 13,866 | 15,960 | 14,266 |
| Total | 255,002 | 248,209 | 232,950 |
Table 1: number of deaths for leading causes of deaths, 2015-2019 (average number) and 2020 (number) and 2021 (number)
The numbers for many, but not all, causes of death fell in 2020 and 2021, compared to the previous five years. In most cases the falls were small, 10% or less, but for influenza and pneumonia, perhaps the most likely candidates to be trumped by covid, the falls were 28% (2020) and 42% (2021). Curiously, the numbers of lower bowel cancer deaths increased in both 2020 and 2021 compared to the previous five years, as did deaths from symptoms, signs and ill-defined conditions. Overall, there were 6,793 less deaths from these causes in 2020, and 20,052 less deaths in 2021, compared to the previous five years. Dr No suggests this data doesn’t rule out covid–19 trumping other causes, but at the same time, neither does it show beyond doubt that trumping happened. All in all, rather a more or less result…
Where does this leave us? We have 6,183 deaths that can be considered true covid deaths, at least by the lights of the entry on the MCCD. We have around 11k (17k minus 6k, because the 6k will be in the 17k) deaths where there may have been other entries on the part I, but if present, they were discarded, and around 140k deaths that appear to have had pre-existing conditions — defined by ONS as “the last health condition mentioned on the first part of the death certificate (the direct sequence of events leading to death) when it is recorded on a lower line to, and therefore clearly preceding, the coronavirus (COVID-19); and all mentions in the second part” — and yet covid–19 was recorded as the underlying cause of death. We still have no way of knowing how often the trumping of the underlying cause of death by covid–19 was legitimate, and how often it was done to reflect “interests of importance for public health rather than what is acceptable from a purely medical point of view”.
What can we learn from this sorry state of affairs? Clearly, very little about how many people really died due to covid—19, because the covid trumping rules so muddy the waters that is impossible to disentangle real due to covid–19 deaths from those hoovered up by the covid–19 trumping rules. The possible range runs, more or less, from 6,183 to 140k, and the failure to have not the slightest clue of where the real number lies represents a colossal failure of public health medicine. Perhaps that leads to the real lesson: in the face of a pandemic of an infectious disease that comes under the special coding rules, you cannot trust the numbers of deaths to be medically correct, because the numbers are not even meant to be medically correct; instead, they are produced to reflect those mysterious interests of importance for public health — whatever they may be.
Edit 1600 29 Jan 2022: inverted percentages in paragraph under Table 1 corrected (72% to 28%, 58% to 42%).
Fraud. Lying. Crooked through and through. Not you, doc: Them.
One number that doesn’t surprise me is the small number of purely Covid deaths. We know, or we suppose we know, that Covid kills mainly by hastening the death of ill, old people, often in care homes. So it’s hardly a shock that its victims are rarely victims of it alone. How many people over 80, in care homes, don’t have nasty underlying conditions? (Genuine question.)
What if we applied WHO logic to seasonal flu? How many people die purely of flu? (Also a genuine question.)
“How many people over 80, in care homes, don’t have nasty underlying conditions?” Very few – see here for some background data (81.5% of 85+ year olds in Scotland have ‘multimorbitities’, on average 3.62 ‘morbidities’), sound study, but note the methodological problems including definition of a morbidity).
“What if we applied WHO logic to seasonal flu? How many people die purely of flu?” Bizarrely, this is supposed to happen – influenza is one of the infectious and parasitic diseases listed in the trumping rules – but, almost certainly, in quiet non-pandemic times, no one quite gets round to doing it: “Unfortunately, we do not hold analysis showing deaths rates for solely influenza from January 1999 to February 2021” Or perhaps they do, but don’t know that they do. This page makes no specific mention of applying the trumping rules, but that doesn’t mean they weren’t applied. One never really knows with ONS…
Yet again I find myself looking at exactly the same Covid 19 issues as Dr No and coming to very similar conclusions. I discovered the following Dutch public health website that spells out the very point made by Dr No in words of one syllable, namely:-
For reasons of surveillance, the definition of death from COVID-19 differs slightly from the standard way in which a condition is regarded as the (underlying) cause of death. In doing so, the instructions of the WHO are followed. Death from COVID-19 is defined as death from a condition related to COVID-19. This means that COVID-19 is regarded as a cause of death in all cases of natural death where COVID-19 is stated on the cause of death form in the causal chain. Example: When both COVID-19 and a chronic condition are on the cause of death form, COVID-19 is considered a cause of death.
https://www-volksgezondheidenzorg-info.translate.goog/ranglijst/ranglijst-doodsoorzaken-op-basis-van-sterfte?_x_tr_sl=nl&_x_tr_tl=en&_x_tr_hl=en&_x_tr_pto=sc
What really concerns me is the way that ONS try and frame the 140,000 deaths attributed to Covid as if they (or the certifying doctor) have determined that Covid was the underlying cause of death. That is now patently not true when it is clearly the algorithm, determined by the WHO that has determined that Covid was the underlying cause. As Dr No says, because of the way this coding works, we really have no idea how many people have died with Covid as the underlying cause. If you add to the mix the unreliability of PCR testing, it confuses the picture even more.
The recent ONS blog on this subject sums up this very point. If it was an honest, true reflection of how Covid deaths were determined, it would point out exactly how “underlying cause” is derived from the MCCD, rather than lead everyone to believe it was as determined by the certifying doctor.
https://blog.ons.gov.uk/2022/01/26/to-say-only-17000-people-have-died-from-covid-19-is-highly-misleading/
Back in December 2020 I suspected something was very wrong with the numbers being reported and came up with the idea of the Covid funnel.
https://twitter.com/PeterHI09614868/status/1344619778598711297?s=20
So far nothing has changed my mind that this is the case and that the true number of Covid cases, hospitalisations and deaths is far removed from the numbers that are reported. However as has been alluded to before, subterfuge and obfuscation seems to be the name of the game in this so called pandemic.
Peter – “it would point out exactly how “underlying cause” is derived from the MCCD, rather than lead everyone to believe it was as determined by the certifying doctor” – this is a very important point, thank you for bringing it up. A common argument used by the debunkers (it was even used against Dr No recently) is ‘how come some conspiracy rando on the internet thinks they know more about the (underlying) cause of death than the doctor who certified the death, and in most cases knew the patient?’ But this misses the point: it’s an ONS rando who re-assigns the underlying cause by applying the the covid-19 trumping rule, not the certifying doctor, that ultimately decides the underlying cause. Usually, doctor knows best, but when it comes to coding covid-19 deaths, ONS knows best.
Thank you Dr No for making this clear. I had made the same error as the biologist you quoted, thinking the 17k over 22 months referred to deaths where covid–19 was the only cause mentioned.
The other colossal failure of public health has, of course, been the political choice to persist with prolonged measures guaranteed to increase population susceptibility to adverse Covid-19 (an other non-Covid health) outcomes (lockdowns, gym closures, stopping team sports, criminalising various outdoor pursuits, school closures) leading to weight gain, worse diabetes control, increased alcoholism, fatty livers, physical de-conditioning, social isolation, social divisions, lack of Vit D, adverse mental health outcomes, anxiety (a risk factor for severe Covid)) etc etc
It would have been really important to know how many of the 6183 or 17k people who sadly died of Covid-19 were overweight or obese. Morbid obesity probably does get included on death certificates, but for a number of reasons, obesity generally does not, and overweight probably never.
How much did we spend on Covid-19 pandemic advertising? In two years I have never heard any of the CMOs or any of the govt spokespeople in any of the daily briefings mention the importance of good nutrition, maintaining a normal weight, good sleep, good mental health, exercise, social cohesiveness and Vit D. Not once. Just masks, isolation, alcohol gel, vaccination and targeting of anyone who for whatever reason is not seen to follow ‘the rules’.
Helen – the errors are easy to make, because of the duplicity (same data appearing in different places in slightly different format or using slightly different criteria) and at the same time opacity of the data. What is not excusable is a flagship BBC Radio 4 programme which claims to make sense of statistics getting basic facts wrong. Why Haffers chose a molecular biologist, who has probably never seen an MCCD, and may be unfamiliar with the formal concept of the underlying cause of death, to research the 17k number is a mystery.
Obesity has been the almost literal elephant in the room throughout the pandemic. Dr No remembers that back in the spring of 2020, before the caring and sharing habit of publishing photos of those healthcare workers who had died from covid thankfully stopped, how struck he was by the apparent prevalence of obesity (and BME background) in those who had died. Maybe they are both more common in healthcare workers anyway, but even so, the observation was striking, and of course, it has since become clear that both are associated with more severe and fatal outcomes.
Unfortunately there is no way of knowing how many of the 17k (which includes the 6k) were obese or overweight. By ONS definitions, these deaths either had only one entry in Part I, presumably covid-19 in some shape or form, or if there was another entry, it wasn’t recorded as a pre-existing condition, and so effectively disappeared.
Of the around 140k who ONS determined died due to covid and with (a) pre-existing condition(s), 2,684 (2%) had obesity (ICD-10 E66, which includes overweight and obesity) listed as a pre-existing condition. Since the prevalence of obesity, especially in those dying from/with covid-19, is orders of magnitude higher, there does indeed appear to be serious under-reporting at work here. All we can really conclude is that it seems highly likely the stats don’t accurately reflect what actually happened…
“Nonetheless, these 6,183 deaths were true (insofar as the MCCD records the death) covid–19 deaths”.
Except that, as I recall, the “rules” laid down by the UK government in March 2020 stated that, from then on and only in cases of Covid, a single doctor could sign a death certificate without having attended or even met the patient.
Thus someone could die, a random doctor could be contacted by phone or email, and that doctor might sign a death certificate saying that Covid was the cause of death – without even knowing anything of the patient’s medical history.
Or have I got something wrong?
Now consider the immense pressure to attribute as much illness and death as possible to Covid – ranging from the penalties, official and unofficial, for disobeying “rules” and “guidelines” to the substantial monetary rewards for toeing the line.
Tom – here is the guidance on completing MCCDs in the ’emergency period’ in full (as published on April Fools Day 2020):
+++++++++++++++++++++++++++++++++
2. Who should certify the death?
In an emergency period, any doctor can complete the MCCD, when it is impractical for the attending doctor to do so. This may, for example, be when the attending doctor is self-isolating, unwell, or has pressure to attend patients. In these circumstances, it may be practical to allow a medical examiner or recently retired doctor returning to work to complete the MCCD.
There is no clear legal definition of “attended”, but it is generally accepted to mean a doctor who has cared for the patient during the illness that led to death and so is familiar with the patient’s medical history, investigations and treatment. For the purposes of the emergency period, the attendance may be in person, via video/visual consultation, but not audio (e.g. via telephone). The certifying doctor should also have access to relevant medical records and the results of investigations. There is no provision in the emergency period to delegate this statutory duty to any non-medical practitioner.
Where the certifying doctor has not seen the deceased before death they should delete the words last seen alive by me on.
If the deceased has been seen before death by a doctor but not the certifying doctor, as well as signing the MCCD they should include the name of that doctor on the MCCD.
In hospital, there may be several doctors in a team caring for the patient. It is ultimately the responsibility of the consultant in charge of the patient’s care to ensure that the death is properly certified. Any subsequent enquiries, such as for the results of postmortem or ante-mortem investigations, will be addressed to the consultant.
In general practice, more than one GP may have been involved in the patient’s care and so be able to certify the death. In the emergency period, the same provisions to enable any doctor to certify the death prevail in general practice.
If no doctor has attended the deceased within 28 days of death (including video/visual consultation) or the deceased was not seen after death by a doctor, the MCCD can still be completed. However, the registrar will be obliged to refer the death to the coroner before it can be registered. In these circumstances, the coroner may instruct the registrar to accept the certifying doctor’s MCCD for registration.
Where a cause of death cannot be ascertained, the death cannot be certified, and the doctor should refer the death directly to the coroner with any supporting information. The coroner may from this information determine no investigation is needed and inform the registrar that the death can be registered. This information will be used for mortality statistics, but the death will be legally “uncertified” if the coroner does not investigate and make a determination as to the cause of death. However, once the registrar has received the coroner’s notification the death may be registered.
+++++++++++++++++++++++++++++++++
The opening and the penultimate paragraph are the critical bits: any doctor can complete the MCCD, and there is no absolute requirement for any doctor to see the patient in 28 days before death/after the death: an MCCD can still be completed, but the death will be referred to the coroner, and yet may still be accepted. This appears to allow any doctor to complete the MCCD, though Dr No has to say that were he in line to complete an MCCD on such terms, he would decline, on the grounds that his powers of clairvoyance were insufficient to divine the cause of death (and so the patient would definitely become a coroner’s case, unless another doctor with better powers of clairvoyance felt able to complete the MCCD).
Putting it another way, Dr No hopes (but can’t of course know) that the vast majority of UK doctors are aware of the limits of clairvoyance as a means of determining cause of death, and so would decline to use it. That said, there was that early report of a Berkshire coroner (who is not necessarily a doctor) who, on hearing the deceased, a young woman, might have had a bit of a cough, promptly signed her off as a covid death.
And yes, guidelines, pressures, hot stuff bias and toeing the line all play their part, but on ‘substantial monetary rewards’ Dr No has to call order. The way UK doctors are paid means there are no substantial opportunities for cashing in on covid, if any. Other influences yes, but not monetary ones.
I wonder what the criteria are for a Doctor to certify Covid-19 as the sole cause of death, with no other health conditions mentioned on the Death Certificate.
What symptoms, and for how long and how severe, did they witness? Or could they rely solely on a positive Covid test?
I wish the over 6000 Covid- only deaths could be analysed by symptoms, because otherwise how can we know what the certifying Doctor is referring to?
Does the 6000 + figure mean anything really?
Isabelle – the criteria are, in effect, to certify the cause of death “to the best of their knowledge and belief”, using whatever clinical and lab data they have available. In general, and this includes covid-19, there are no condition specific criteria, eg there is no requirement to have a positive PCR test result (clinical suspicion is sufficient) – and of course, a positive PCR isn’t necessarily proof that covid-19 was the underlying cause of death. But, if it walks like a duck and talks like a duck, and, on top of that, there’s a lot of it about…which is to emphasise yet again that even when the certifying doctor knows the patient, establishing the cause of death is not an exact science.
“Does the 6000 + figure mean anything really?” The answer is both yes and no. It means there were 6,183 deaths in which the certifying doctor (who may or may not have known/seen the patient) believed “to the best of their knowledge and belief” (sharp readers will already have smelt the whiff of tautology at work here) that the deceased had died from covid-19, and only covid-19, and with no other (pre-)existing conditions. But because of the caveats, we have no way of knowing how accurate this diagnosis was, and so have to take the number with a large pinch of salt, to the extent that in effect it becomes meaningless.
That said, it is worth noting in passing how infrequently (4% of all covid-19 deaths) the certifying doctor believed, to the best of their knowledge and belief, that covid-19 was the sole cause of death.
Looking at the very helpful Table 1, I notice the steep falls in pneumonia and flu. The average decrease for 2020 and 2021 appears to be 8-9,000 per year. Whereas the number of indubitably, indisputably Covid deaths was 6,000-odd for both years combined…
Hmmmmm. I can imagine two things, one of which fits comfortably inside the other.
By the way, Dr No, I think I see a typo:
“…for influenza and pneumonia, perhaps the most likely candidates to be trumped by covid, the falls were 72% (2020) and 58% (2021)”.
As far as I can see, the figures were 72% and 58%, corresponding to falls of 28% and 42%.
Tom – thank you, well spotted. Now corrected.
Reading Dr No’s article and all ensuing comments inevitably leads to the question:-
“Does Covid 19 actually exist as a new and novel disease, or is it just a re-branding of illnesses that have always existed in the past ?”
I believe it is now becoming clear that the claimed number of deaths, with Covid 19 as the underlying cause, has been seriously overstated. However, after listening to many front line doctors, eg Dr Peter McCullough, who have actually treated so called Covid patients, it also seems that these doctors do clearly believe there is indeed a previously unseen, atypical respiratory disease called Covid 19.
I have been trying to find an explanation from an unbiased respiratory specialist what, other than +ve PCR, the key, clear cut, clinical differences between “genuine Covid” and other respiratory illnesses actually are, but as yet have been unable to answer this question. Maybe Dr No can help here. (Hypoxia and blood clotting do seem to be key characteristics. Could these be a response to some form of toxic agent rather than a virus ?)
My current view (but I am open to be persuaded otherwise) is that Covid 19 does exist as an atypical respiratory disease, but to a far lesser extent than we have been led to believe, with case, hospitalisation and death numbers being ramped up through conflation with other illnesses.
So if Covid 19 does exist, albeit in much smaller numbers, for me the question still remains what is causing it ? I’m afraid I remain unconvinced by the natural virus narrative (See Dr No’s blog on Macavity the mystery virus)
Not that my opinion is worth a light but I’m currently of the view that this disease is probably due to some synthetically engineered nanoparticle, or maybe even some other as yet unknown mechanism.
@PH: figure 2 at this link supports something I’ve thought for ages: there really was a nasty spike of excess deaths in the Spring of 2020. If doctors are at the same time reporting unusual modes of death (such as Dr Kendrick did) then I reckon there was indeed am epidemic. But has there really been one since? Figure 2 leaves the question open but perhaps inviting the answer “no”.
https://dailysceptic.org/2022/01/28/latest-mortality-figures-suggest-that-vaccine-effectiveness-has-been-overestimated/
I’ve enjoyed this chap’s book about his brief spell at the White House as a pandemic advisor. I suggest it might be wise to watch this YouTube before the buggers censor it.
https://www.youtube.com/watch?v=v3i8HXKHISA
dearieme – great video, but not necessarily the one you meant to link to?
Ya got me bang to rights, doc. Less musical but more Covidical:
https://www.youtube.com/watch?v=t6kmm70ji5c
On the same subject, did you see this?
https://www.statsjamie.co.uk/medics-misleading-on-child-covid-deaths/
(links to the original BJGP opinion piece)
Has there ever been a time when clinicians have held such strongly held diametrically opposite beliefs about health? No one I work with thinks this way. I know where, and how, our perspectives have diverged, but I don’t know how, or if, we’ll ever reach a point of shared understanding.
Helen – there’s something of an epidemic of ‘official’ misinformation going on, much of it focused on kids. Suffer the little children etc. As well as Louise Hyde’s inflated death counts (which she has now corrected), there are a number twitter threads eg this one ratcheting up coviparanoia focused on children, some using dodgy data, others using emotional language. To their credit, other contributors have been very level headed, but the general movement appears to be towards more rather than less polarisation, with children being used to heighten the emotional tension.
A question if I may, doc. (You’ve probably discussed it already but perhaps before I started following your blogging.)
A plots of excess deaths against time make it clear that we had a nasty little epidemic in the Spring of 2020. But that came after the usual flu season.
Was there a normal flu season in, say, November 2019 – February 2020?
dearieme – there are many different ways of measuring the flu season. Consultations? Media hysterics about A&Es being overwhelmed? Admissions? Laboratory diagnoses? Flu deaths (and if so, how decided)? Excess deaths? All cause deaths? All cause mortality is the most robust, and all cause deaths are easier to get and look at (with excess deaths, there is always the question of excess compared to what? Recent say last five average? Non flu season deaths etc). Excess winter deaths are sometimes used to assess a flu season, but usually cover December to March, and so for 2019 – 2020 includes (and so is inflated by) covid deaths. So we need to look at weekly deaths.
With those caveats out of the way, there was a ‘normal’ (though a bit smaller than in some recent years, both in height and width) hump in excess deaths during winter 2019 – 2020 before covid arrived, perhaps most easily seen in this chart from PHE’s Surveillance of influenza and other respiratory viruses in the UK Winter 2019 to 2020 (curiously, the current 2020 to 2021 one doesn’t cover mortality). Though PHE uses EuroMOJO’s dreaded algorithms, the chart does show weekly deaths (solid black line) and the ‘corrected’ is benign, just ironing out bank holidays etc.
The PHE report, by the way, contains a lot of additional data, worth looking at for a fuller picture, if the fancy takes you.
From The Times:
“Fences at all of Britain’s National Hunt racecourses will be repainted white, after scientists found that horses could not properly see the orange traditionally used.”
Apparently we use evidence-based actions to protect horses. Pity we don’t do the same for people.
Towards the end of this piece there’s a fine moan from a practising US physician about the failings of the CDC.
https://www.nakedcapitalism.com/2022/02/just-scandalous-cdc-withholding-most-of-the-covid-data-it-gathers-what-is-it-trying-to-hide.html