
The Needle and the Damage Done
“Even the perpetrators had to go one step at a time, completing each step before they realised that the next one was possible.” Clive James, Review of Holocaust (BBC1), 1978 Whither Covid Vaccines? Yesterday, Secretary of State for Health Sajid Jabbit confirmed in the Commons that Covid vaccination will be compulsory for all frontline NHS staff in England by next April. Rumour has it that J-Day will be set for the 1st April, an unfortunate choice, raising the question of whether Jabbit is a joker, or a fool, or perhaps even both. Certainly the Royal Colleges and Unions are up in arms, pointing out that banning qualified healthcare workers from working — a sure fire way to make enemies and alienate people — at a time of NHS crisis is foolish in the extreme. Many, including Dr No, have questioned the ethics of mandatory healthcare worker vaccination, but this is a tricky one, because of vaccine precedents in healthcare, even if those precedents were, and remain, a condition of employment, rather than a legal requirement. And then, last but by no means least, there is the prickly question of the medical evidence: do covid vaccines reduce the risk of covid transmission?
The medical evidence is crucial, because the whole edifice of mandatory covid vaccination for healthcare workers rests on the premise that the vaccines reduce secondary transmission. If they do, then a case can be made that perhaps covid vaccination should indeed be made a condition of employment for front line staff. If they can’t be shown to reduce the risk of transmission, then the whole edifice comes tumbling down, and Jabbit’s gambit stands revealed as gratuitous authoritarianism, without even the slightest medical, let alone ethical, justification.
There are two ways a vaccine can reduce transmission. The first is by reducing infections in vaccinated people — less cases means less transmission. The second is by reducing infectiousness in breakthrough infections: those who get infected despite being vaccinated are less infectious, because they have been vaccinated. The two ways are not mutually exclusive, a vaccine might reduce the number of infections, and make the breakthrough infections less infectious. Equally, the vaccine might fail on one or both counts. We need to look at both to determine whether or not a medical basis exists for mandating covid vaccination for healthcare workers.
The first question, does vaccination reduce cases, is the easy one to answer, and the answer is they don’t. For the last several weeks, the UK Health Security Agency’s weekly covid vaccination surveillance reports have consistently shown that covid infection rates are higher in those that have been jabbed than those that have not, across all ages in those aged 30 and over. For those aged 18 to 29, which will include a lot of healthcare workers, infection rates are marginally higher in the unvaccinated, but, as with other age groups, the trend over time has been more infections in the jabbed, and less in the un-jabbed. Under 18 year olds are a striking, and unexplained, exception. The latest data are shown in Figure 1. These are based on large numbers from national surveillance, and are unlikely to be wildly inaccurate, despite heroic attempts by UKHSA claiming that we really shouldn’t worry our silly little heads about these data, on account of ‘underlying statistical biases in the data’.
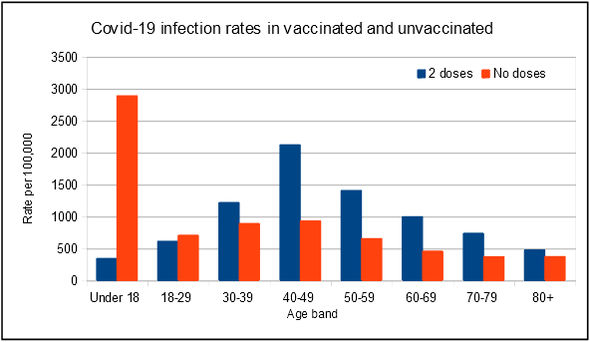
Figure 1: covid infection rates (strictly speaking, PCR positives) in England by age band for double vaccinated and unvaccinated individuals, for weeks 40 to 43 in 2021. Source: UKHSA
Data on the effectiveness of vaccines against transmission in breakthrough cases are far more sparse. This is perhaps not surprising, because what we are looking for here is not how well the vaccines protect the person vaccinated, but how well the vaccines protect others from those who are infected; in other words, in the language of the mask wars, we are interested in source control. Specifically, we need a classic cohort study that identifies a cohort, in this case index cases, classifies them by exposure to the factor of interest, in this case vaccination, and then follows up the cohort over time to determine how many events, in this case onward transmission, occur in each group. Modern epidemiologists can’t resist muddying the waters by doing fancy analyses using stochastic Rubik cube transformed inverse Bayesian models based on impenetrable formulas incomprehensible to man before presenting their results, but at the heart of any cohort study lies a very simple two by two table. The two rows are exposed and not exposed, and the two columns are had, and didn’t have, the outcome of interest. For a cohort study on smoking and lung cancer, the rows are smokers and non-smokers, the columns are those who got lung cancer, and those who didn’t. The results compare the attack rate (lung cancer rate) in smokers and non-smokers.
These rates are the crude, unadjusted rates, but they remain at the core of any cohort study. Often there is a need to adjust the figures: for example, let us imagine that all smokers were aged 60 and over, and all the non-smokers were aged 16 and under, then we would need to adjust for age, which we can do mathematically, or more transparently by stratifying (grouping) by age. But the principle of a cohort study remains the same: we compare the event/outcome (infection) rates in an exposed (vaccinated) group to the rates in the unexposed (unvaccinated) group.
Cohort studies by their nature are labour-intensive, expensive, and time consuming, and don’t often get done, as the underwhelming result sets from searches for ‘covid secondary attack rate in vaccinated‘ and ‘covid vaccine effectiveness transmission‘ on Google Scholar reveal. Furthermore, the studies need to be relatively recent, to cover delta covid, and to ensure adequate numbers of fully vaccinated individuals in the population. Some of the papers display an alarming lack of understanding of basic statistical principles — misuse of standard deviation is a classic, as in ‘The average age of the study population was 33 years (standard deviation 19.4)‘ which means a significant minority of the study population had yet to be born (mean 33, SD 19.4, 95% of the ages fell in the range –5 to 71) — and these papers can be confidently spiked without further ado. A number of others had woefully inadequate follow-up. Two linked Dutch studies, for example, had subjects who were ‘encouraged to get tested‘ and ‘urged to get tested‘, which don’t quite cut it as rigorous follow-up. Others fell to the spike because the data collection ended before delta covid predominated, and vaccination became commonplace. Several studies have appalling attrition rates, with hundreds of thousands of potential subjects yielding actual subjects in the single thousands, if that, raising major questions of selection bias. And finally, far too many papers fail to report the raw numbers; and to put it bluntly, Dr No is always sceptical if all you can see is the results after they have been through the modelling kaleidoscope.
One often quoted letter — it is not even a full paper, but it does include some raw numbers — reports SARs (secondary attack rates) of 10.1% for unvaccinated index cases, and 5.7–6.2% for vaccinated index cases, but, crucially, fails to describe how contacts were followed up, and so we have no idea how biased (or not) the reported rates are. Furthermore, the study ran in England from 4th January to 28th February 2021, when only highly selected groups, the over 80s and clinically vulnerable, had vaccinated, and delta covid had not yet arrived, and so cannot be extrapolated to today’s circumstances. Thwack! Another report hits the spike!
Dr No had high hopes for this paper, but yet again it falls foul, by failing to provide adequate follow up. In a commendably clear and open discussion, the authors say ‘We considered only contacts who underwent PCR testing… Therefore, we cannot estimate secondary attack rates by case and contact vaccination status’. The crucial point, and the reason why so many papers end up spiked, is that if you do not achieve comprehensive follow-up contacts — that is, all tested, and all results recorded — then you have no way of knowing the true secondary attack rates. It is the age old eight out of ten cats, or in this case, three or four out of ten contacts problem: the full statement should read three or four contacts, of those who got tested, tested positive.
Instead of spiking yet more inadequate papers — by now, it should be clear most studies do not include sufficient data to allow true secondary attack rates to be estimated — let us now turn to the only two studies Dr No has found that do have sufficient raw data and clear confirmation of adequate follow-up. Neither are perfect, and numbers are small, sometimes painfully so, but they the best we have got, and most interestingly, they produce almost identical results, despite being done in very different settings, at opposite ends of the earth. The results replicate each other, a key test of scientific validity. Without further ado, let’s cut the crap, and go to the two by two tables that lie at the heart of these cohort studies.
The first study was done in Singapore, which accounts for the thoroughness of follow-up. Date collection ended at the end of May 2021, but they still managed to include 753 delta cases, and Table 3 reports the raw numbers of secondary cases in close contacts by index case vaccination status. The second study, which appears to be an epic attempt at obfuscation on account of the primary findings being not quite what the doctor ordered, was done in England, and the second (ATACCC2) arm, which we are interested in, ran from May to September 2021 in London and Bolton, where delta covid was common. The authors are to be commended for the rigour of their follow-up, and Table 2 reports the raw numbers of secondary cases in close contacts by index case vaccination status. The results from both papers are presented in Table 1 below. To keep things simple, only the unvaccinated, and the fully vaccinated, are shown.
| Singapore | PCR+ | PCT- | Total | SAR |
| Index case vaccinated | 29 | 109 | 138 | 21.01% |
| Index case not vaccinated | 127 | 425 | 552 | 23.01% |
| England | PCR+ | PCT- | Total | SAR |
| Index case vaccinated | 17 | 52 | 69 | 24.64% |
| Index case not vaccinated | 23 | 77 | 100 | 23.00% |
Table 1: crude (unadjusted) secondary attack rates among contacts in Singapore and England by vaccination status of the index case. PCR+/PCR- is the number of PCR positives/negatives among contacts of the index case, SAR is the secondary attack rate (percentage of contacts who get infected for that row)
The numbers, particularly in the English study, are painfully small, meaning wide open confidence intervals and low statistical power (the ability to determine a difference, if it really exists), and they are crude rates, but nonetheless, the secondary attack rates are all remarkably similar. Unless and until better data emerges — and readers are cordially invited to submit anything they have found in the comments below — Dr No suggests that this is the best indication we have so far of the ability of vaccines to control onward transmission of delta covid, and the answer, with the caveats noted above, is that it appears they don’t limit transmission. Vaccinated or unvaccinated, it makes no difference, the SAR stays the same.
This means, on the basis of current evidence, there is no scientific basis for mandating covid vaccination for frontline healthcare workers. It also means, of course, that covid vaccine passports are meaningless. Individuals remain free to chose vaccination to protect themselves, if that is what they wish to do, but the idea that vaccination and vaccine passports can provide source control is for the time being dead in the water. Jabbit’s diktats aren’t the caring actions of a Secretary of State hoping to protect vulnerable patients, they are another step among the deplorable consequences of gratuitous authoritarianism. Come to think about it, if staff on the wards need vaccine passports, how long before visitors on the wards also need vaccine passports? My, oh my, the needle and the damage done.
It’s always good to channel Neil Young!
Great post! – but how to get this (and all the other sensible information) to the idiots in thrall to this nonsense.
‘Come to think about it, if staff on the wards need vaccine passports, how long before visitors on the wards also need vaccine passports? ‘ At the latest, the day after, because, let’s face it, we’d better act fast to stop kovi…. Like, April Fool’s Day 2022… Like, next year… As in, 4.5 months from today… Which means, doesn’t it then, everyone will be six feet under after the massacre microscopic particle’s increasing onslaught, which requires compulsory pricking of the entire population of planet-eco-dying-itself-earth (step by step, in lockstep) to stop said massacre of its inhabitants… Yea, right, Jabbity Javid.
Clothes peg please; the rats are stinking more than is bearable by surely ANYone now!?!
Is it possible that there’s something in the vaccine that’s being picked up in PCR tests? Looks like the positive test rate has doubled for those vaccinated first.
If being vaxxed/unvaxxed makes no difference to transmission I suppose it’s reasonable to guess that the same would be true of boosted/unboosted.
OK, so no need for me to take a booster to protect my wife. But I’m still waiting to see much about the efficacy and safety of a booster for me. I’d have hoped for a flood of papers. What’s Up, Doc?
Ed P – how indeed? But looking at the data, and getting it out there, as in Table 1 in the post is a start, but not enough. We are against entrenched views, of the ‘being Aryan is best’/’being vaccinated is best’ order. Some vaccines work well, some (mostly respiratory ones) don’t work well, and it increasingly looks like covid vaccines fall into the latter group. But the fanatics don’t want to see it that way, and the government, already drunk on power, are more than happy to use any pseudoscience to push through gratuitous authoritarianism. Wait and see: the ‘Come to think about it, if staff on the wards need vaccine passports, how long before visitors on the wards also need vaccine passports?’ that Annie picked up on is the penultimate sentence in the post for a reason (and the last is really Dr No’s way of trying to both wrap up the post and acknowledge where the title came from, because anyone who knows the song will know recognise the word order).
The idea that the vaccine might of itself somehow trigger a positive PCR test is probably impossible to rule out, but it is extremely unlikely, for a number of reasons, including some rather murky virological ones (presumed fragility, incompleteness and short life of the vaccine products), and perhaps rather more persuasively, the epidemiological one, waning immunity. If the vaccines were triggering the positive PCR tests, that effect should decrease over time, but what we see is the opposite.
All of this is muddied further by lack of data on what counts as ‘a case’ after vaccination. Did the Dutch subjects who were ‘urged’ and ‘encouraged’ to get a test (and who knows who did and didn’t heed the urging and encouraging) get tested regardless of symptoms, or were they always symptomatic, or both? Almost all of the studies have this fatal flaw (incomplete follow up) which is why Dr No zoomed in on the two that do have adequate followup.
dearieme – there is no semantic difference between vaxxed/unvaxxed and boosted/unboosted, so your reasonable guess makes sense. The reasons for the lack of a flood of papers are many. No doubt not wanting to piss on one’s own parade is apart of it, but the pragmatic one is that doing proper follow-up studies, which are the only ones that will give definitive answers, is demanding in time effort and money. As time goes by, and more people get vaccinated, they also become harder to do, because you have less unvaccinated people to study. Recall, if every one smokes, it is all but impossible to do an epidemiological study that proves smoking causes cancer, because you have no control group.
Government policy is the driver of all things, there is no or very little thinking going on.
The policy is double jab or perhaps triple jab now we have a so-called booster.
It’s still easy for the Government to sound as if they are correct with their double jab mantra. This is partly because most people don’t have the time to do their own research and humans will tend to trust the main or in this case only narrative from main stream media.
My wife who trusted the overall message had her two jabs, as did my son. What happened, she caught covid in September, probably from my son. I caught it too, and as a no jab person seemed to get off more lightly than my poorly wife. No evidence to see here but perhaps an interesting anecdote.
Her decision is not to have a booster because she now thinks we were sold a pup.
Trust of the Government does seem to be wearing a bit thin, and I do wonder whether this giant propaganda machine will be found out.
Meanwhile, on planet curious, a Swedish study has found some evidence the S Spike protein may damage a cell’s DNA repair system in some way. As far as I know this was only in vitro and the paper has not been peer reviewed. So, that’s okay then!
By the way, we were always told the so-called vaccine does not and could not affect the nucleus….
Spike Protein Goes to Nucleus and Impairs DNA Repair (In-Vitro Study)
Dr Mobeen explains with some lovely diagrams.
Many thanks for this, Dr. No. It seems the needle can be damaging in other ways. Retired Nurse Teacher Dr. John Campbell has picked up the fact that jab deliverers in both UK and US no longer aspirate the syringe as once was done as a matter of course, thereby checking that they have not hit a blood vessel where you definitely don’t want this particular substance delivered. It would seem the current cohorts of health care workers have been told that aspiration of the needle is unnecessary!?
Campbell explains here:
https://youtu.be/nBaIRm4610o
Infection control requires 100% single barrier protection. It doesn’t matter whether just some Jibby-Jabbers are infectious and/or some just a bit infectious – that is not infection control and a fail. (Same for masks, distancing and hand sanitisation rituals carried out at alters in shop doorways,)
The infection still can be transmitted and since different people, whether Jibby-Jabbers or Jabby-Dodgers will respond differently, it doesn’t matter how reduced the number of infectious or how reduced their infectiousness, the end result will be the same, continued random, unstoppable transmission and varying degrees of disease including hospital admissions and death.
And speaking of infection control failure: The Prime Directive of infection control is – Do Not! mix infectious people with non-infected people and certainly not in the general hospital population, given what bug breeding grounds hospitals are. Yet they have done just that right from the start, and doctors and nurses (all genuflect and clap) have remained silent on this fundamental issue. It’s science, Jim, but not as we know it.
In fact from what I read, even the uncritical mush pushed out in the MSM, vaccination doesn’t perform any better in suppressing transmission or degree of infectiousness, nor seriousness or death then the unadulterated immune system.
As for making next April the execution date, if it is so vitally important would not right now be the essential time to do it going into the Winter when cases of SARS, ‘flu Colds are going to increase?
Delaying until Spring – when SARS will go quiet – is like sending the Fire Brigade to a house fire in 6 months time.
The only conclusion is it is a move determined by politics, or rather saving embarrassment, from a seasonally busy NHS which can’t cope not because too many cases, but too few staff who aren’t working because they refuse vaccination.
Could the higher number of ‘cases’ in the teens & young adults be an artefact created by that group having more tests so they can go to watch football, visit night clubs, play sports, etc?
It would really be nice to know how many of each age group actually are admitted WITH/BECAUSE OF CoVid so we can put the ‘case’ and ‘infection’ numbers in perspective, because there seems to be quite a miss-match between these tens of/hundreds of thousands of ‘cases’ and hospitalisations and deaths.
When I lived in Australia I was assured (by someone in a position to know) that NHS infection control was poor by the standards of other advanced countries. Is this still true?
I ask as someone whose FIL was killed by an MRSA infection picked up in an NHS hospital.
Seen in the blogosphere: “The only way we will be able to make informed decisions about vaccination in the future is by monitoring adverse events. A vaccine mandate, if effective, would eliminate the control population, making it impossible to determine whether adverse events are due to the vaccine.” Oh dear.
https://mises.org/wire/unfortunate-consequences-bidens-vaccine-mandate
H/T The Daily Sceptic
dearieme – this is very true. An essential part of any cohort study or clinical trial is the control group: you compare the outcome rates (either good or bad or if you are doing it properly, both) in the exposed (to the treatment/noxious agent/whatever) to the outcome rates in the unexposed group. No control group, no comparison, no result. Studies such as these become impossible when everyone is exposed to whatever it is (if everyone in the population smokes, you can’t use epidemiological methods to find out if smoking causes cancer).
That said, even a universal vaccine mandate (it may only be a matter of time before we see one here in the UK) will still leave some unvaccinated, so all is not lost, though it may well be that the unvaccinated are an ‘unusual group’ in more ways than one…
‘Come to think about it, if staff on the wards need vaccine passports, how long before visitors on the wards also need vaccine passports? ‘ …
…Today, Esther Rantzen coolly declared on GB News that (she thinks) older people who refuse a (third) vaccination, and become ill for whatever reason, should stay home and die rather than be hospitalised, because they have chosen not to ‘follow The Science, as we say’.
Shocking that we find ourselves here so soon. I think we spoke of slippery slopes once before, but when you see what is happening globally (Australia, New Zealand, Lithuania, Austria etc), I’d say we’re on a hell slide right now and I feel sick in my stomach.
Your appraisal of the evidence is appreciated. I’m always hopeful that science will triumph over The Science. Other studies that call mandates into question are listed here: https://brownstone.org/articles/20-essential-studies-that-raise-grave-doubts-about-covid-19-vaccine-mandates/
So as far what science appears to be telling us is:
1. Both vaccinated and unvaccinated people can acquire and transmit infection.
2. Once infected, there is no difference between vaccinated and unvaccinated people in terms of infectiousness (SAR/CT values/viral load)
3. Viral loads may drop marginally more quickly in vaccinated people but at peak infectiousness (when it counts) they are identical.
4. You cannot know a person’s immune status (and risk of acquiring and passing on infection) from their vaccination status. To do so risks over-estimating (in those whose immunity has waned or who didn’t mount a good immune response) or under-estimating (in those who are unvaccinated but prior infected, recovered, immune) their immunity.
5. Prior infection confers superior immunity to vaccination-acquired immunity.
6. Vaccination-acquired immunity wanes and may be as low as zero (or lower..).
7. It is currently anticipated that repeat boosters will be needed to maintain immunity against current infections. We don’t currently know how often people will be called on to take one for the team.
8. Repeated vaccination against a very selected part of the virus will lead to selection pressure on the virus.
9. Other variables influencing individual vaccine-acquired immunity include immune response to the vaccine (all the risk factors for severe Covid are risk factors for poorer vaccine response), time since last vaccine, general health (eg obesity is a risk factor for increased symptoms, increased viral load, transmissibility).
10. Symptomatic healthcare workers are very good at taking a test and staying at home. This is the single most important action for an infected person.
11. Asymptomatic transmission is less common than symptomatic transmission. Pick a number, any number. Let’s go for an upper level of 25-28%. I think that is a high estimate, but depends, as with symptomatic transmission, on the nature of the contact. As symptomatic workers will be at home, this is the crux of the vaccine mandates, that we are unknowingly potential vectors.
12. Vaccinated people may be more likely to be pauci-symptomatic or asymptomatic than unvaccinated (though are we confident about this? Locally I see little difference in presentation by vaccination status).
13. Households, hospitals and care homes are the highest risk settings for transmission.
14. A study in Cambridge suggested that hospital-acquired infection usually comes from other sick patients not from healthcare staff.
15. Reports vary globally and may depend whether early or late in a ‘wave’ – Sometimes we see more unvaccinated Covid positive people in hospital (earlier?); Other times more vaccinated (later?). Not sure what to make of hospital data as hard to know how many have symptomatic Covid versus incidental positives.
16. Risk of severe infection/hospitalisation and death remains low in low risk people (on age/health grounds), though is higher now in pregnant women than it was previously.
17. It seems that more infectious variants predominate since global mass vaccination. I don’t know if the CFR is increasing. Some say it is, which would be highly unusual unless there is some pressure to select for more virulence; some say it isn’t.
18. Social connectivity and behaviour matters (more contacts, more close contacts, more household contacts = increased risk) as does the nature of the contact (indoor/outdoor, how close, how long, ventilation).. A vaccinated social butterfly with poor immunity/poor health/obesity is potentially at higher riskier of acquiring and transmitting infection than a shy single (healthy) unvaccinated person. Some of these risks can be mitigated.
19. There are confounders in all studies purporting to measure vaccine efficacy and there are different motivations for individual testing (unvaccinated kids testing like crazy in school; some vaccinated people may not be testing as they tell themselves it’s just a cold; many vaccinated aren’t as afraid as they were so don’t bother testing).
20. Vaccine mandates lead to the resignation and sacking of valuable workers.
21. Our health and social care services are chronically understaffed. There is no slack in the system.
Science seems to be telling us that, on current empirical evidence, vaccine mandates aren’t going to benefit the population. They most certainly will cause harm, by adversely affecting staffing ratios and causing back pressure on hospital beds, ambulances response times etc.
Let’s face it, all doctors now know first-hand that vaccines don’t stop infection, and yet…
…even though science is telling us this, The Science emphatically still backs mandatory vaccination, segregation, sacking and social death of unvaccinated people.
I’m curious as to why this is so, even in the face of all that now appears blindingly obvious (to me, to others). I’m no psychologist, but want to understand. Is this is a case of ‘moral dumfounding’, where belief in The Science underpinning vaccine mandates and medical segregation, is actually based on reflexive, intuitive and emotional judgement and not on evidence-based public health?
A problem arises if scientific understanding matures to a point where it potentially undermines the moral case for mandates. The post-hoc rationalisation used to defend such a position will become increasingly incoherent, but you/I/we will never win the argument through reason. In order to maintain the position of moral superiority and to avoid dissonance, would it be necessary for those who embrace vaccine mandates, sacking of healthy workers and generalised ideals of vaccine apartheid, to obscure, deny, deflect, minimise and cancel all reference to vaccine harms?
I wonder, is there any evidence that this is happening?
A nasty thought has occurred to me. I see blog posts alluding to the unusually high rate of heart problems among young athletes who are assumed, by the bloggers, to have been vaxxed. That the rates are unusually high may just be an assumption too.
But suppose the bloggers are right on both counts and, further, that the vaxxes are the cause of the problem. My nasty thought is that heart damage in these cases would be unusually conspicuous since the victims are otherwise healthy, super fit, young, and famous. What if such heart damage also occurs among the rest of us but is simply less conspicuous? Would the effect be “lost in the noise” unless a deliberate effort were made to search for it?
Sounds logical to me, dearieme. After all, older people do get heart attacks, don’t they? And strokes. probably because they are so lazy, sitting on their couches watching TV, and eating all that dangerous red meat…
Yes, and there may be a reason as to why some people, mostly the young and male are getting Myopericarditis.
Dr John Campbell has highlighted a potential problem, which has reported on his excellent YouTube channel. The reason is that we no longer aspirate an intramuscular injection. There is therefore a potential to inject intravascularly… Which is not where this needs to go!
Inadvertant intravenous injections
Intravenous Injection of Coronavirus Disease 2019 (COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse Model
From his video, in bullets;
Background
Post-vaccination myocarditis and pericarditis reported after coronavirus mRNA vaccines.
The effect of accidental intravenous injection of this vaccine on the heart is unknown
Methods in mice: compared difference between i.m. and i.v. injection of vaccine
Clinical manifestations, Histopathological changes
Tissue mRNA expression
Serum levels of cytokines and troponins with normal saline (NS) control
Results
Intravenous SARS-CoV-2 mRNA Vaccine Administration Induced Grossly Visible Pathology in Heart
Only IV group developed histopathological changes of myopericarditis
Evidenced by cardiomyocyte degeneration, apoptosis
Necrosis with adjacent inflammatory cell infiltration
Calcific deposits on visceral pericardium
But
Evidence of coronary artery or other cardiac pathologies was absent
Spike antigen (immunostaining) occasionally found in infiltrating immune cells of the heart
And in cardiomyocytes and intracardiac vascular endothelial cells
The histological changes of myopericarditis after the first IV-priming dose persisted for 2 weeksand were markedly aggravated by a second IM- or IV-booster dose
Numerous inflammatory cytokines found in cardiac tissue (interleukin (IL)-1β, interferon (IFN)-β, IL-6, and tumor necrosis factor (TNF)-α)
in the IV group but not the IM group compatible with presence of myopericarditis in the IV group
Ballooning degeneration of hepatocytes was consistently found in the IV group.
All other organs appeared normal.
Conclusions
In vivo evidence that inadvertent intravenous injection of COVID-19 mRNA vaccines may induce myopericarditis.
Brief withdrawal of syringe plunger to exclude blood aspiration may be one possible way to reduce such risk.
Both Pfizer/BioNTech and Moderna have clearly stated that their vaccines should only be given via IM route
Current CDC and WHO guidelines no longer recommend precautionary measures during IM vaccine administration
The CDC Pink Book 2020 and WHO 2015 position paper have recommended against aspiration prior to vaccine injection so as to minimize pain
Deltoid to the vastus lateralis? Our study indicates that IV injection of vaccines might partially contribute to this clinical phenotype, thus warranting a reconsideration of the practice of IM injection without aspiration, which carries the risk of inadvertent IV injection.
Thrombocytopenia in mice reported in 2006
Steve – have taken the liberty of removing some of the white space, hope that’s OK.
I’ve just found this, which has come to the same conclusion – the myocarditis and whatnot in young athletes may indeed also be shared by the rest of us.
https://stevekirsch.substack.com/p/over-a-60x-increase-in-serious-adverse
He refers to this paper which has been disappeared.
https://www.sciencedirect.com/science/article/pii/S0146280621002267?via%3Dihub
The WaybackMachine still has the abstract of the disappeared paper. It concludes ‘COVID-19 injectable products are novel and have a genetic, pathogenic mechanism of action causing uncontrolled expression of SARS-CoV-2 spike protein within human cells. When you combine this fact with the temporal relationship of AE [adverse event] occurrence and reporting, biological plausibility of cause and effect, and the fact that these data are internally and externally consistent with emerging sources of clinical data, it supports a conclusion that the COVID-19 biological products are deterministic for the myocarditis cases observed after injection’. Not the most lucid of prose, but we get the drift.
Helen – thanks for such a comprehensive comment. “I’m curious as to why this is so, even in the face of all that now appears blindingly obvious (to me, to others). ” This is something that has bothered Dr No almost from the start of the pandemic. He has made a few forays into possible explanations in past posts, with what happened in 1930s Germany as an obvious starting point. A highly developed sophisticated modern society managed a race to hell in a bare few short years. How on earth did that happen? Some observations:
‘The Science’ (Aryan superiority) was created by and led by the medical profession. Sure it was music to Nazis ears, who were already thinking along those lines, but ‘The Science’ itself came from (medical) ‘scientists’. The quotes are present because these ‘scientists’ were anti-scientists, doing the opposite of science. They had beliefs, and then cooked up some ‘evidence’ to back up their beliefs.
It seems modern societies are both extremely susceptible to the influence of any science, and at the same time are incapable of distinguishing true science from bad science. This may be because (a) humans have a tendency, even a need, to ‘believe’ (in something, even anything) and (b) most modern humans have little or no understanding of science (sceptical, questioning) vs The Science (dogmatic, insistent). Humans, it appears, would rather believe in a creed, even if the creed is wrong, than live in a world of intellectual challenge and consequent uncertainty. Many Germans believed in Hitler’s creed, and that he would lead them to better things. It is always more pleasing to believe you are going somewhere, rather than nowhere.
The toxic lynchpin: create a fear of and then an incensed rage against an enemy within. This allows (Freudian) projection to happen at a societal level. Society spilts, and then fractures, and the process becomes self-fuelling, like a nuclear reaction. This is the point of no return: once crossed, the society will descend into an ever deeper and darker hell until it utterly and completely destroys itself. We are on the cusp of that point right now, right here in Britain, which is why so many of us get so worked up about things like mandatory vaccination and vaccine passports. They are the machinery that carries society over that point of no return.
The above was written yesterday (Sunday). Overnight, it has emerged that Austria, another ‘highly developed sophisticated modern society’ has all but introduced a yellow star scheme. ‘Covid: Austria introduces lockdown for unvaccinated: Unvaccinated people will only be permitted to leave home for limited reasons, like working or buying food’.
Reaction on twitter? “Why should anti vaxxers enjoy the freedoms that the vaccinated people have technically afforded them?” “Selfish narcissistic anti-vaccers are clogging up the NHS. How dare they seek treatment” “Lockdown the unclean” Consider these, and then re-read the paragraph one before last. The machinery that carries us past the point of no return is already beginning to turn.
There are two books which I’ve read and go into some detail about beliefs and mass movements.
“Why We Believe What We Believe” by Andrew Newberg and Mark Robert Waldman. This tends to look at the neurology of beliefs, brain structures etc.
The True Believer (Thoughts on the Nature of Mass Movements) by Eric Hoffer. Considers the bigger picture and how people align or become true believers to the cause.
I suspect all Governments and some scientists have well thumbed copies!
Dr No, we all very much appreciate your perspicacity.
I was heartened recently to hear the following statement given by another (old school) doctor:
Dr Iona Heath CBE FRCGP, Ex President of the RCGP (November 2021):
‘I am 71 years old and I was grateful to have been vaccinated against Covid-19. I have four grandchildren aged between 10 and 14. Every working day in Primary Care I have seen how the theories of Medicine work themselves out in the lives of individuals and families, and this experience has reminded me, repeatedly, of the provisional nature of knowledge. As time goes by, theories, knowledge and certainty all come and go. The new drug that is greeted as a miracle is condemned as a poison a few months or years later.
None of us can be certain about what the future will bring.
I have long thought that one of the most important roles of a Primary Care Physician is to protect patients from the harms of Medicine, because we are committed to seeing and hearing each person in the fullness of their context and biography, and we know that the body is not a machine, and because we work at the frontline of Medicine, at the point where science and life-experience intersect.
Medicine becomes dangerous, whenever the lives, context, hopes and priorities of individual patients are lost from view; whenever healthcare becomes depersonalised by Public Health Utilitarianism on a macro-scale and/or by biomedical scale on a micro-scale. Many of the people we have heard from today, have been squeezed between both these modes of depersonalisation. Their individuality has been lost from view, and their experience has been discounted.
Listening to their stories I have been powerfully reminded of a paper written by David Sackett 20 years ago, which had a very striking title, ‘The Arrogance of Preventive Medicine’. In it he wrote, ‘Preventive medicine displays all 3 elements of arrogance. First, it is aggressively assertive, pursuing symptomless individuals and telling them what they must do to remain healthy. Occasionally invoking the force of law (immunizations, seat belts), it prescribes and proscribes for both individual patients and the general citizenry of every age and stage. Second, preventive medicine is presumptuous, confident that the interventions it espouses will, on average, do more good than harm to those who accept and adhere to them. Finally, preventive medicine is overbearing, attacking those who question the value of its recommendations.’
I am confident that you can see why I thought of this paper, by someone who has been described as the Father of Evidence Based Medicine. Extraordinary things seem to happen to people in power, when they begin to believe that fear can only be contained by absolute certainty, very much along the lines of, ‘Accept this wonder vaccine. It will stop you dying and it will do you no harm, or only harm of a most trivial nature.
But people are not stupid. They know full well that life and death are full of uncertainty. They also know that fear is contained, not by certainty but by trust. It is a tragedy for all of us, that the devastations of the current pandemic come just at the time that the extent of corruption in the Medical Industrial Complex, by powerful vested and financial interests, has become undeniable and has made trust very hard to come by.
All those who have suffered harm from vaccines, all the children for whom the risks seem to outweigh benefit, and all those whose livelihood and social interconnectedness are being threatened by vaccine mandates, are being asked to pay too high a price for the false certainty of those who think they can predict the future.
When British playwright Harold Pinter won the Nobel Prize for Literature in 2005, he said this: ‘I believe that despite the enormous odds which exist, unflinching, unswerving, fierce intellectual determination as citizens, to define the real truth of our lives and our societies is a crucial obligation which devolves upon us all.’
I think that this is what we have been trying to do today, and I thank you all.’
LIVE IN D.C.: EXPERT PANEL ON MEDICAL MANDATES & VACCINE INJURIES Doctors & medical researchers treating COVID-19 vaccine injuries gather with vaccine-injured patients to discuss the growing problem
Helen – thank you for these wise words from Iona Heath. Among other things, they also bring to mind The Death of Humane Medicine and the Rise of Coercive Healthism by Petr Skrabanek. The common theme is that doctors should always consider their patients as autonomous individuals, rather than automatons in a bigger machine, to be manipulated at will be the authorities. The Germans tried that in the 1930s, and it didn’t end well.
Following on from what Steve mentioned, and many others, and even though I had heard Prof Mattias Desmet before (and know about ‘mass formation’), I found this fascinating indeed – even if nearly 90 minutes long. (Sorry for the long link, but my bet is Dr No can carry out a neat bit of cosmetic surgery on it!) Operation done, link here.