
Ode to the Death Certificate
Covid! The very word is like a bell, to toll me back from my sole self to thee! Dr No continues to wonder about covid entries on death certificates, and how and why these entries do or don’t end up in ONS’s weekly counts of covid deaths. Unlike the pin-ball wizardry of counting every single death within twenty eight days of a positive covid PCR test as a covid death — an indiscriminate and robotic definition — one hopes, rather forlornly, that a modicum of medical effort on the part of the doctor completing the medical certificate of cause of death, or MCCD, followed by sensible coding of underlying cause of death by ONS, might give confidence that when we sidestep Donne and send to know for whom the bell tolls, then at least the count of tolls for covid are reasonably accurate. But are they?
The principles of death certification, and recording the cause of death, are simple enough. The MCCD has on it two boxes, one for recording the cause of death, and another for recording contributing conditions. In the cause of death box, there are three lines, and the general idea is that the top line records the immediate cause of death, and subsequent lines any conditions that lead to the condition in the line immediately above, with the lowest entry being the underlying cause of death. The aim is to record the chain of events that led to death, rather than just the immediate cause of death. For instance, a diabetic individual might die from a myocardial infarction (a heart attack), which was caused by ischaemic heart disease. Myocardial infarction would be entered on the first line, as the immediate cause of death, and ischaemic heart disease on the second line, as the underlying cause of death, and it is this underlying cause, the condition that initiated the train of events that ended with death, that will show up in ONS cause of death statistics. Diabetes would go in the second box as a contributing factor, rather than taking a place in the chain of events that lead to death.
The general idea is to record the most meaningful cause of death. A person might die from internal bleeding (the immediate cause of death), but the information becomes more meaningful when we know that the bleed happened from a ruptured major arterial blood vessel, with the rupture caused by a road traffic accident. In this case, road traffic accident would be recorded as the underlying cause of death, which in turn led to arterial damage, which in turn led to the patient bleeding to death.
ONS regularly report that, give or take a few percentage points, of all deaths that involve covid, where covid appears anywhere on the death certificate, around 90% are found to have covid as the underlying cause of death. This means these deaths will be counted as a covid death. This strikes Dr No as a little counter-intuitive, given that the vast majority of covid deaths happen in the elderly and very elderly, and that, unsurprisingly, many of these poor folk also have many other non-trivial medical conditions. How reasonable is it to say that someone knocking on heaven’s door who is pushed over the threshold by covid, as the final straw that breaks the camel’s back, is truly a covid death? On one level it is true: covid did push them over the threshold. But it is also true that covid could only do that because of the pre-existing underlying conditions, and the general principle in coding causes of deaths is that the underlying cause be recorded as the cause of death. If a patient dies from bronchopneumonia, caused by immobility and wasting, themselves caused by Alzheimer’s disease, then the underlying cause, and the one that will be coded as the cause of death by ONS, is not bronchopneumonia, but Alzheimer’s disease.
There is an element of semantics going on here. Strictly speaking, to be in box 1, a condition must be part of a chain of events where one leads to another, implying a causal relationship. In the Alzheimer’s disease example, which by the way comes from longstanding official guidance, Alzheimer’s disease led to immobility which then led to bronchopneumonia. On the other hand, a patient made frail by a long term condition, and so vulnerable to severe (and then fatal) covid–19 infection appears to fail to meet the strictly causal chain of events requirement that would make the long term condition the patient’s underlying cause of death. Or does it? What if we re-word the events: the patient had a long term condition that led to frailty and vulnerability that allowed, enabled, or even led to covid–19 infection, and subsequent death? This wording, which closely echoes the Alzheimer’s disease example, does provide a sequence that appears to satisfy the chain of events requirement, such that the underlying long term condition, and not covid–19, was the true underlying cause of death.
To understand what is going on, Dr No first reviewed once again the post covid arrival revised government guidance on completing death certificates. Immediately something appears to be at odds with normal practice. Putting aside the word salad in box 1 (c), and the messy layout, the guidance gives this example of a correctly filled in MCCD with COVID-19 as the underlying cause of death:
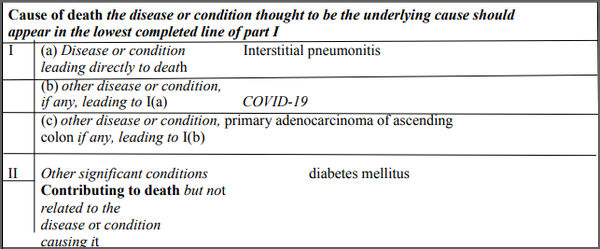
Recall that normally the lowest entry in box 1 (in this case, primary adenocarcinoma of ascending colon) will be the underlying cause of death. In this case, a higher entry, covid–19 on the line above, has trumped, as underlying cause of death, a clearly potentially lethal condition, colon cancer, that has been entered by the certifying doctor in the place normally reserved for the underlying cause of death. How can this be?
ONS is somewhat opaque on how it actually codes deaths. It uses ‘automatic cause coding software’ with names like IRIS and MUSE, which it updates from time to time. Nonetheless, the general gist of its coding operation appears to be in line with WHO guidance, and is based in ICD-10, the current version of the widely used International statistical classification of diseases and related health problems. As well as listing the classification of diseases, ICD-10 also has Volume 2, an Instruction Manual which, among other things, contains ‘practical instructions for mortality and morbidity coders’. Here, if anywhere, we will find the general principles and rules governing the coding of deaths, including, presumably, those used in ONS’s coding software.
Volume 2 was published before the arrival of covid–19. Soon after the appearance of the new virus, WHO issued additional guidance on the certification and coding of covid–19 as cause of death, and this is where things start to get interesting. The guidance defines deaths due to covid–19 rather vaguely — basically, in the absence of an obvious alternative cause, if it looks like covid–19, then it is covid–19 — and then states (emphasis added): ‘A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of pre-existing conditions that are suspected of triggering a severe course of COVID-19′.
This bit of the guidance is crucial. It basically says that once covid–19 has been identified as the cause of death, using the rather slack ‘if it looks like covid, then it is covid’ criteria, then it trumps any other cause of death, and the death gets counted as a covid–19 death, even when there are pre-existing conditions that may have triggered severe covid–19. This flies in the face of the general principles for identifying the underlying cause of death, which should be the lowest entry in the cause of death box on the MCCD. Covid–19, should it appear higher up in the list, takes over, and becomes the underlying cause of death — just as happened in the example given above from the UK guidance, and, we have to presume, given the example given in the image above is official government advice, happens as ONS codes covid–19 deaths.
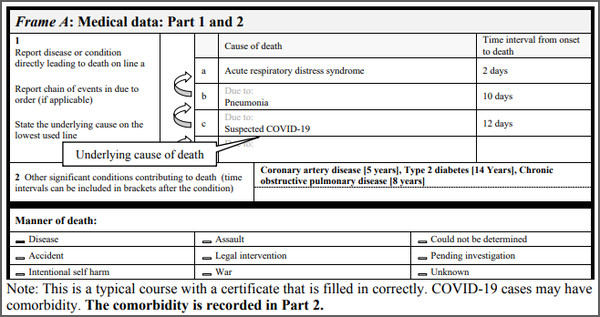
This can only have one effect: to inflate covid–19 deaths. An individual dying of lung cancer, or any other cancer, or chronic non-communicable respiratory disease, or renal disease, or whatever, who gets pushed over the edge by covid, gets counted as a covid–19 death. The pre-existing conditions, however serious and significant, are instead to be demoted to box (Part) 2. The guidance is clear: ‘If the decedent had existing chronic conditions, such as these, they should be reported in Part 2 of the medical certificate of cause of death’, leaving King Covid reigning supreme as the underlying cause of death. Even a full house of long-standing and nasty co-morbidities can conveniently be disposed of, as this example from the guidance shows:
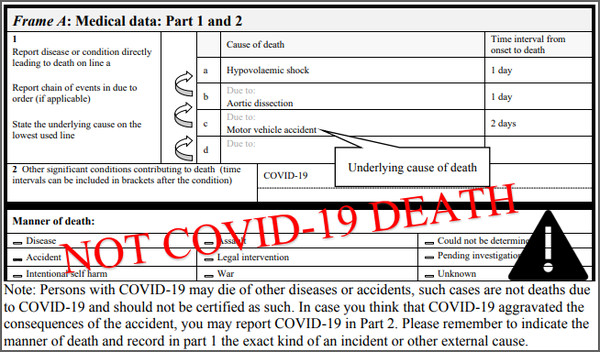
Reluctantly, and almost as an afterthought, the guidance does concede that people ‘may die of other diseases or accidents’, even when they had coincidental covid–19, providing the other cause is overwhelmingly obviously not covid–19. Examples given include myocardial infarction (heart attacks) and road traffic accidents:
The rational for this guidance — that most of the time, unless there is a barn door alternative non-covid–19 cause, covid–19, once present on a death certificate, will trump all other causes and get counted as the underlying cause of death — is the ‘intense public health requirements for data’ and the need to ‘produce the most useful cause of death statistics possible [reflecting] interests of importance for public health rather than what is acceptable from a purely medical point of view‘. Indeed, so intense is the requirement that coders are ordered to ‘always apply these instructions, whether they can be considered medically correct or not‘ [emphasis added].
Put simply, this part of the guidance justifies cooking the books in the interests of public health. A case can be made, which Dr No might even tolerate, though not support, along the lines that desperate times call for desperate measures, if the rules used for coding were made widely and freely available, and were presented alongside the data they had shaped. But they are not. Instead, the data have become the ‘most useful’ statistics that reflect public health and political interests, rather than ‘medically correct’ data. This stinks of propaganda, and the weaponisation of statistics. Wordsworth’s nightingale of truth has just flown away, and the dark and lamentable shadow of deception has darkened our doors.
It’s almost as if there’s a worldwide plan to inflate the figures…except in China, where very few have died with/from covid. (Either they’re suppressing the death figures, or they have contained an infection the rest of the world has handled very badly.)
Most people now know masks are ineffective, as are lockdowns.
Normal seasonal flu has all but vanished, as have colds.
Our lying ‘leaders’ must be challenged and brought to justice when (if ever) this debacle is over.
I have been waiting a long time for someone to write of this; back in March I read the official guidance and was tempted to write something myself, but decided that I lacked the medical knowledge to make practical sense of it.
One observation re: ” ‘A death due to COVID-19 may not be attributed to another disease”
I thought that when in March the ONS started giving a separate figure for COVID deaths it was to meet this requirement, but that with as in the official example above (Covid in box 1b) the detail of the true underlying cause would be preserved so that when the final and fully coded figures were published (usually in August of the following year) it would be possible to see the true state of affairs. But it seems this is not going to happen, the figures are irredeemably compromised.
djc – Dr No also initially hoped ‘all would be revealed’ when the full cause of deaths stats came out in due (but still a long time after the event) course, and then realised as you have that the data has been compromised at the most basic level, the completion of the MCCD. The coding rules certainly aggravate the compromise, but if the basic data, the entries on the MCCD, are already biased, there is no going back to true reality.
The situation is not helped in the least bit by ONS’s opacity on how it actually codes deaths. The inference on its methodology page is that it follows WHO guidelines (and frankly it would be rather surprising if it didn’t), but we don’t know if it has tweaked anything. The guidelines say this is a no-no (because the whole idea is to be able to make international comparisons) so we can only assume that ONS does follow the WHO rules to the letter.
In one foolish reverie the other day Dr No imagined ONS might one day publish some identity redacted MCCDs to show exactly how it coded covid-19 and other deaths. Fat chance…
My thoughts when I heard the 90% statistic were that they must simply count any mention of Covid in Part 1. I think that during a pandemic if there’s a whiff of Covid then your average Dr is putting it somewhere in Part 1. So essentially you will always die of Covid if you’ve had a recent positive test or a cough or many other symptoms depending on the opinion of the certifying Dr.
“… one hopes… that a modicum of medical effort on the part of the doctor completing the medical certificate of cause of death, or MCCD, followed by sensible coding of underlying cause of death by ONS, might give confidence that… the count of tolls for covid are reasonably accurate”.
Dr No, as a layman I wonder how easily a doctor could decide whether a person had died of Covid (or even “with” Covid), given the great overlap of signs and symptoms with other common diseases.
It seems that official guidance encourages doctors, even those who sign a death certificate, to keep at a distance – and I understand that post mortems, for example, have been positively forbidden in cases where Covid is even suspected.
But even if a doctor attended a dying person until the moment of death, and were able to examine the patient, how easily could she be expected to distinguish between Covid and flu, for example? Or pneumonia not associated with Covid? Or even TB?
For such purposes I suggest that the popular DNA/RNA tests should be discounted, as they are so inaccurate – and a person with a positive test may not show any signs or symptoms of Covid.
I suggest that, as you mention, the key issue is simply that governments have decided – quite arbitrarily – to treat Covid on an entirely different footing from all other diseases.
That is just one of the disastrous consequences of allowing officials and politicians to make important medical decisions.
Shawn – covid anywhere in Part 1 = covid death is pretty much what the WHO rules add up to. Also agree about any whiff of covid = covid in Part 1 (this is hot stuff bias at work). End result: lots and lots of covid deaths.
Tom – “one hopes…” – Dr No added “rather forlornly” partly to acknowledge Wordsworth (the actual lines for those who don’t know them by heart is “Forlorn! the very word is like a bell, To toll me back from thee to my sole self!”) but also because it is a forlorn hope: bedside diagnosis of the cause of death is notoriously unreliable, and positive (or indeed negative) PCR tests do nothing to help. All we are required to do as the doctor completing the MCCD is to do so “to the best of [our] knowledge and belief” and you are absolutely right, in the mish-mash of overlapping symptoms and signs it is not at all easy to be sure what is and isn’t the cause of death (except in obvious cases, like a silver dagger through the heart – but even that may not be what it seems, and anyway will become a coroners case, and so will get a PM). The reductions in the requirements that need to be met before completing an MCCD can only have made the accuracy of the diagnosis of cause death even more uncertain. If we add that plus WHO and governmental public health and political motivated tinkering with the certification and coding process together, we have the ideal conditions to create pandemic wildfire of deaths that will burn out of control as it spreads round the globe. Which is pretty much what happened…
http://www.nrscotland.gov.uk/files//statistics/covid19/covid-deaths-21-report-week-02.pdf
Very interesting article – thank you.
The data for Scottish excess deaths on page 10 of the link to the NRS website above supports your assessment of the situation Dr No. Excess deaths recorded in hospitals as due to Covid are more than balanced by a deficit in records of deaths due to cancer, dementia, coronary heart disease etc. One good thing is that at least the NRS report has some transparency in this respect.
Carol – thanks for the link, and the pointer to page 10. Figure 4 on that page is telling and worth repeating here:
Dr No has been looking at similar data for ICU admissions and while there is a similar pattern (other causes for ICU admission down as covid goes up), the effects are less pronounced. This may well be because of bias eg who does and doesn’t get selected for ICU, and is not easy to tease out, though age and prognosis are likely factors.
Dr No. I saw this today – an analysis of ONS all mortality figures by Dr Darko Butina (retired research chemist), 2020 stats set against all years from 1953 and in line with population growth – 17 million between then and now. Overlooking hyperbole header by the Liberty Beacon, he sets out his workings very clearly:
https://www.thelibertybeacon.com/shocker-new-official-data-exposes-uk-lockdown-lies/
Tish – Dr Butina’s heart is in the right place, but he didn’t do the sums quite right, he mixes up rates and numbers (counts), and doesn’t provide all the sources he used (unless Dr No missed something). He also missed out the need to age standardise, ie account for changes not just in the size, but the structure of the population (more or less older people etc).
He uses the UK population as the denominator, E&W deaths as the numerator (divides E&W deaths by UK population rather than E&W population). Not a grave error, and an easy mistake to make (Dr No has made similar ones), but nonetheless…
He says “However, if you compare the UK population in 1953 to 2020, you will notice that the year 2020 has 17 million more people than 1953 and therefore larger annual deaths rate. (emphasis added)”. This should be “However, if you compare the UK population in 1953 to 2020, you will notice that the year 2020 has 17 million more people than 1953 and therefore larger annual number of deaths“. The rate has actually gone down…
Dr No’s post Early Assessment of 2020 Mortality shows the importance of age-standardising. The blue line in the chart at the top of the post is the equivalent of Dr Butina’s line (only E&W deaths/E&W population), ie crude mortality per xxx population, and the green line shows what happens when you add age standardisation (ie account for more older people. Here’s the chart again for quick reference:
As you can see, adding age standardisation makes one hell of a difference.
I will add this comment to Dr Butina’s post pointing these things out. His post has value if it helps folk understand how the necessary adjustment that need to be made, but it is still worth doing them correctly!
PS Should also add Dr Butina’s chart is what is known in the trade as a Gee-Whizz graph (Y-axis doesn’t start at zero, has the effect of exaggerating any apparent trend).
Many thanks for unravelling this, Dr. No.
It’s not Wordsworth, it’s Keats.
Theodore – Dr No is indebted to you for correcting what was a terrible mistake.
There’s an interesting post here about covid deaths in the Republic of Ireland (not a lot to see here, on the basis of all cause ASMRs), with a convincing suggestion that those alleged to be covid deaths may in fact have been stolen from other causes of death because of the ‘covid trumps all’ rule for coding deaths. Long post, but a recommended read.