
Macavity The Mystery Virus
“And when you reach the scene of crime — Macavity’s not there!
You may seek him in the basement, you may look up in the air —
But I tell you once and once again, Macavity’s not there!”— T. S. Eliot, “Macavity: The Mystery Cat”, Old Possum’s Book of Practical CatsPerhaps the greatest problem facing modern science isn’t the corrupting influence of power and money, but an even deeper one of incomprehensibility. Dr No has touched before on how increasing super-specialisation means that increasingly scientists from one discipline are unable to make sense of another discipline, because the language and theory in each discipline have become so dense as to be impenetrable to all but initiates in that discipline. It is as if science has become a broad church spreading its wings over a vast array of cults and sects, each one swearing allegiance to the Greater God of Science, but each with its own rules and creeds, an impenetrable vista of numberless caverns of knowledge meaningless to man.
Take virology, for example. Not by a long shot the medical student’s favourite subject, the average doctor will qualify with vague notions of tiny obligate intracellular parasites — see, the language is already dense — some of which infect humans and cause a host of diseases, some mild, some middling, and some truly terrible. In time, it will dawn on the doctor that almost all viral diseases cannot be cured by medical science, and with that dawning, the need to understand the basic medical science of virology recedes still further. Instead, the doctor has to take it on trust that the white coats in the virology labs know what they are talking about. And therein lies the problem: take it on trust is anathema to science. One could even go further, and say it is the Anti-Science.
This impenetrability of super-specialised basic medical science has been rudely brought to the fore by the arrival — or not — of SARS-CoV-2. Because the vast majority of practicing doctors haven’t a clue about modern virology, they have to take it on trust that the virus exists, and causes covid–19. Next time you see a doctor, ask him or her this: how do we know that SARS-CoV-2 exists, and causes covid–19? You will get as many different answers as doctors you ask, but all will share a common theme: that we have to take it on trust that all those papers reporting the isolation, culture and genomic description of the virus stack up. Push the average doctor further, and it will rapidly become all too clear that he or she has not the slightest clue about the science behind that stack of papers; instead, he or she has had to take it on trust that the science is sound. But this is the opposite of science. If a scientific claim cannot be understood and verified, then it is not science. Take it on trust based medicine isn’t evidence based medicine, it is cult based medicine, wherein the acolytes of the cult believe without question the creed of their cult.
In the beginning was the virus, and the word was with the virus… It is all too easy to see how this sort of nonsense will very quickly lead to claims that the virus is no more than the apple in Dildo Harding’s eye that will become Bramleys in her bank account. Indeed, Dr No has been asked many times about the evidence for the existence of SARS-CoV-2, and its role in causing covid–19. His response was to collect some of the key papers that claim to have demonstrated isolation of SARS-CoV-2 — for example, this one from CDC, and this one from McMaster, with a ‘lay’ version here — and see what sense he could make of them. The result is a long post, but by the end you should have a better understanding of where we really are with SARS-CoV-2 and covid–19.
Pretty soon, he came up against the concrete wall of super-specialisation. Not long after, he suspected that, as Doctor Who once said, he had reached the point where his brain tissue was ‘so massively hybridised that the next metabolic change could be the final one’. How else to respond to CDC’s ‘We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL’, or McMaster’s ‘We maintained Vero E6 cells (African green monkey cells; American Type Culture Collection) in Dulbecco’s modified Eagle medium (DMEM) supplemented with 10% fetal bovine serum (FBS) and 1× l-glutamine and penicillin/streptomycin’? Eye of newt, and toe of dog…like a hell-broth boil and bubble. Eye of cow and toe of monkey — virology, it turns out, is a modern form of ancient witchcraft! A hell-broth of animal remains, fetal extracts and modified mediums, laced with a potent cocktail of antimicrobials! Double, double toil and trouble!
Still massively hybridised, but narrowly managing to avoid the next metabolic change ‘that could be the final one’, Dr No at last deciphered some of the witchcraft. It took one hell of a while, but it can be done — at least, Dr No thinks it can. Although both papers talk of isolating the virus, it is not isolation as we normally understand it. The methods described do not lead to a vial of pure SARS-CoV-2. Instead they produce a hell-broth culture that, through the logic of modern virology, is said to be infected with SARS-CoV-2. Viruses, recall, are obligate intracellular parasites, meaning they have to infect cells to be able to grow. You can’t just cut and paste some SARS-CoV-2 onto a Petri dish, and hope to come back the next day and find lots of little SARS-CoV-2 jobbies swimming around in the agar. Until they become inside jobs, they remain elusive — Macavity viruses.
Even today, we might note in passing, the freely available vials of ‘isolate’ contain not pure (‘isolated’) virus, but rather ‘cell lysate and supernatant from [insert cell line of choice here: human lung cancer cells, monkey kidney cells, eye of newt or toe of dog] infected with SARS-CoV-2′. Cell lysate is the result of, for want of a better description, the chemical liquidation of cells, by breaking down the cell outer membrane. The ‘isolate’ may well contain some SARS-CoV-2, but it also contains a lot of other material, so much so that the term ‘isolate’ is a misnomer.
The next two steps in ‘isolating’ the virus are critical to understanding the process. The first is to establish that the virus is pathogenic, that is, it causes cell damage. The cell lines used in viral culture are already on life support — that’s why all the mediums and antimicrobials are present — because they have to be immunodeficient, to allow the virus to grow unchecked. To test for pathogenic effects, the virologists run two cell cultures, one inoculated with the suspected virus, and the other with a mock inoculation, and then observe the cultures over time. If so-called CPEs, or cytopathic effects, are seen in the suspected virus culture, but not the mock inoculation culture, then the virologists conclude that there was something in the suspected virus sample that caused the cell damage, and presume that it was the virus. But they don’t know. Maybe the cells is the suspected viral culture started checking out for some other reason.
At this point, it is worth viewing the key figure in each paper that shows the cytopathic effects. Note the inclusion of the mock inoculation — in effect a control — because a common criticism of SARS-CoV-2 viral culture studies is they don’t include controls. Anything could have cause the cytopathic effects, all the more so given the hell-broths used in the cultures. The truth is that at least these two studies did use controls. The cells only started checking out in large numbers when the suspected virus was present.
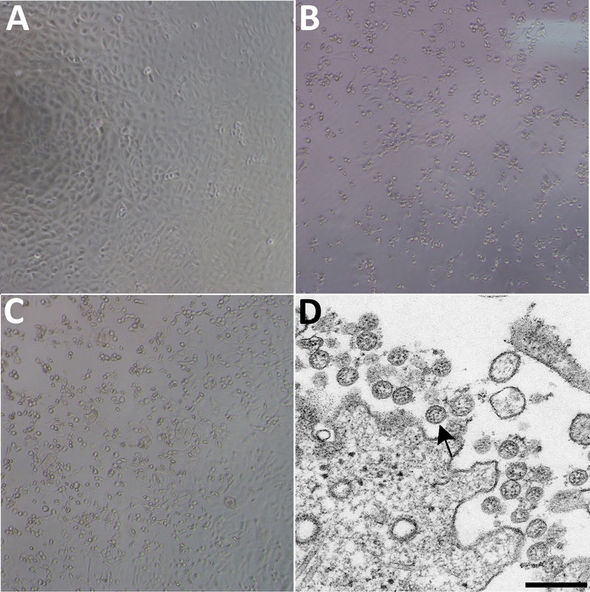
Figure 1 (CDC): Figure 1. Cytopathic effect caused by severe acute respiratory syndrome coronavirus 2 from patient with coronavirus disease, United States, 2020. A–C) Phase-contrast microscopy of Vero cell monolayers at 3 days postinoculation: A) Mock, B) nasopharyngeal specimen, C) oropharyngeal specimen. Original magnifications ×10). D) Electron microscopy of virus isolate showing extracellular spherical particles with cross-sections through the nucleocapsids (black dots). Arrow indicates a coronavirus virion budding from a cell. Scale bar indicates 200 nm. Click here for original, larger version.
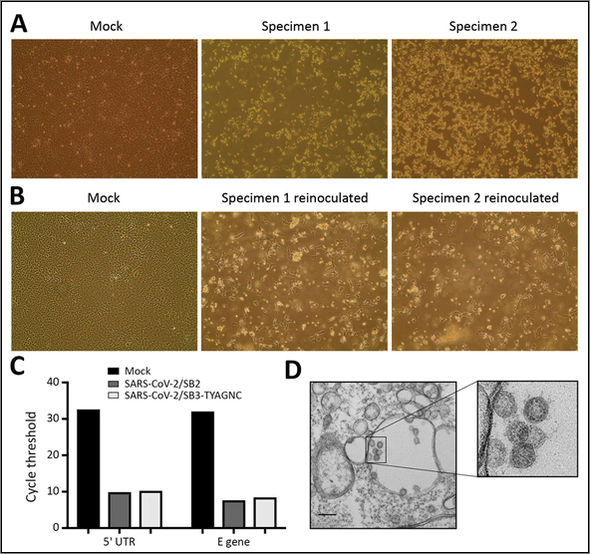
Figure 2 (McMaster): Figure 2. Isolating severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from patients with coronavirus disease (COVID-19). A) Vero E6 cells were mock inoculated or inoculated with midturbinate clinical specimens from COVID-19 patients. Cells were incubated for 72 h and observed for cytopathic effect (CPE) under a light microscope. Original magnification ×10… Click here for full caption and original, larger version.
The two figures also include electron micrographs claiming to show cross-section through ‘extracellular spherical particles’ (CDC) and ‘coronavirus-like particles’ (McMaster). CDC go a big step further and use an arrow to indicate ‘a coronavirus virion budding from a cell’. Nonetheless, Dr No has to conclude that, so far, the studies are satisfactory. Not only have we managed to penetrate the concrete wall of super-specialisation, we have also found on the other side of that wall what appears to be reasonable experiments. There is a rationale for using the hell-broths, and the experimenters did run controls, and perhaps most important of all, each study appears independently to replicate the other. Although published in the same journal, the studies were independent: the CDC one based on a 35 year old male from Washington in January 2020, and the McMaster one on two rather less well defined Canadian samples from early 2020.
The second step in ‘isolating’ SARS-CoV-2 is much murkier. So far, we have ‘a coronavirus virion’ and a ‘coronavirus-like particle’ visible in cultures taken from patients with respiratory illnesses from early 2020. So far so good, were it not for the fact that common cold coronaviruses are endemic in the winter months in the Northern hemisphere. Perhaps Macavity is a common or garden moggy. Perhaps Macavity’s not there!
To solve this conundrum, both studies used PCR tests, the test known locally in this parish as the sewing machine test, on account of its uncanny ability to detect a local working sewing machine based on a fragment of a broken needle discovered in a remote haystack. We can confidently step over that hokum, because it is meaningless, and move on to whole genome sequencing, noting that, in passing, CDC, but not McMaster, ran rapid assays (sewing machine tests) for 33 other respiratory viruses, and found none were present. No needles found, so that’s alright then.
If PCR testing is like trying to zip up a dress when one half of the zip is missing most of its teeth, then at least whole genome sequencing improves your chances, because the entire two halves of the zip are present. But are they from the same zip? This is by far the murkiest area in both studies. The relevant text in both studies is so massively hybridised one more word change ‘could be the final one’. Rather than try to penetrate the impenetrable, which nonetheless emits a faint odour designer genomes (‘we designed’; ‘we generated’; genome sequences were assembled’), let us instead consider the timelines. Both studies appear to rely on the now somewhat infamous early SARS-CoV-2 genome sequences released by the Chinese during the late 2019/early 2020 Wuhan outbreak as their reference genome, CDC’s study on NC045512, and McMaster’s on MN908947.3. Scroll down to see the actual sequence in full — the blocks of attaaaggtt sequences. Then check the submission details near the top. In both, it says: “Direct Submission… Submitted (05-JAN-2020) Shanghai Public Health Clinical Center & School of Public Health, Fudan University, Shanghai, China”. Note the date: 5th January 2020.
When did the Chinese first discover the cause of the previously unexplained Wuhan outbreak was a coronavirus? Reports are murky, but WHO said back in 2020 (the page has since been liquidated) that the Chinese first isolated a coronavirus as the cause on 7th January 2020. Chinese news reports at the time appear to confirm this, saying that ‘as of 21:00 on January 7, 2020, the laboratory has detected a new type of coronavirus and obtained the…whole genome sequence of the virus’ and that the ‘virus was isolated from a sample of a positive patient.’ Yet the same news report also says further down the page that the discovery of ‘pathogenic nucleic acid, genome and antibody evidence from patients can be completed in a short period of time. The isolation of pathogens and the identification of pathogenicity and other scientific research can take several weeks’.
In an eggshell, this is a chicken and the nut problem. Everything is mixed up, as in Dr No’s last sentence. If the isolation of the virus takes several weeks, how did the Chinese manage to have the whole shebang wrapped up by 21:00 on the 7th January 2020, one week after declaring an outbreak (31st December 2019), and only four weeks after the first patient developed symptoms (8th December 2019)? What is the proper sequence of events? How is it possible to sequence a genome before you have isolated the pathogen, and identified its pathogenicity? How can you submit the ‘complete genome’ two days before you have detected the novel virus? Dr No may be being painfully naïve, but it seems to him the first step is to identify the pathogen, using cell culture, and only then sequence its genome. For SARS-CoV-2, both appear to have happened in parallel, or even the wrong way round: sequence then ‘isolate’ and identify. And all of that at an indecent warp speed fast enough to cause Dr Spock’s ears to penetrate the ceiling.
None of this makes sense. Dr No has looked in the basement, and up in the air, slept on the conundrum and pondered in a chair, and nothing has even remotely come to light. He can and does accept the reports that ‘coronavirus-like particles’ have been cultured from patients with respiratory illnesses, but that is as far as it goes. SARS-Cov-2 may well be real, and may well cause covid–19, but unequivocal evidence is either lacking, or so massively hybridised, that it is as if it doesn’t exist. Nothing in the accounts of the PCR testing and whole genome sequencing in the studies even approaches sufficient weight to persuade Dr No that he could, were he called to do so, stand up in a court of law, and hold out a vial to the judge and declare, “that, your Honour, is SARS-CoV-2, and that is what causes covid–19″. If someone who spends most of their time on the opposite side of the concrete wall of impenetrability can enlighten Dr No and his readers, then please, for the love of God, do so. In the meantime, we may have seen a whisker, but in all other respects, Macavity’s not there!
Very interesting. I think your point about super specialisation is very relevant. The loudest voices throughout have come from specialists in areas that most of us had never come across before and prior to recently would never have had a platform to speak directly to the public. I’m very much a generalist and one who’s seen patients continually since the start of the pandemic and that’s left me with a continues sense of living in a parallel reality where I hear one thing from ‘experts’ or ‘leading doctors’ ( who I doubt have seen a patient in years) but with my own eyes I see something very different. Namely I don’t see any Covid. I honestly can’t say that I’ve seen anyone in over eighteen months who I’ve thought, ‘this looks like Covid’. Sure, I’ve occasionally been told at a later date that x has tested positive, but clinically I couldn’t have made a diagnosis. And even the numbers we’ve had testing positive and then needing admission or later dying have been tiny, certainly not what I’d expect from the daily barrage of fear from everywhere. Incidentally, I do believe there is a clinical picture that can identify patients who have severe Covid and are subject to the myriad of investigations that you’d expect if you land up on ITU but without CT scans etc there isn’t any way your average GP is going to make a diagnosis.
Dr Malcolm Kendrick, for long a determined sceptical voice, declared recently that he has given up trying to make sense of the whole Covid-19 affair because it seems impossible to get hold of reliable data. https://drmalcolmkendrick.org/2021/09/03/i-have-not-been-silenced/
Distrubingly, Dr Kendrick writes:
“After reading this, do I still think SARS-CoV2 exists? Yes, I do. I firmly believe that I watched people dying of it, from it. They died in a way I have never seen people do so before, and I have seen a lot of people die. They seemed quite well, then suddenly their oxygen sats dropped like a stone – they still seemed okay otherwise – then they died. The end.
“Very strange, and rather disturbing. I started slipping an oxygen saturation monitor onto my finger from time to time. Just in case. 99% is my average reading, if you are interested. It never dropped”.
Tom, thanks for finding that quote from Dr K – I tootled off last evening to look for it and became distracted. I believe I’m correct in stating that Dr K was, at that point, dealing almost entirely with elderly patients who were either already in hospital or in a care setting? Clearly there was or is some viral thing doing the rounds that is serious for those in a certain age range – or those with chronic underlying health issues – who contract it. How widespread it is now is quite another matter. Are we now spreading something similar but different via vaccination??
Yes, Carolyn, I think that was the case. Back in January and February 2020 Dr Kendrick said he drew up a list of drugs and materials necessary for treating Covid-19, including (from memory) hydroxychloroquine and oxygen as well as protective gear, and was astonished and horrified when the NHS bosses actually vetoed HCQ and joined the ventilator stampede.
Anyone could be forgiven for getting sucked in to Dr Kendrick’s blog, as he has done so much fascinating research (or perhaps I should say “study”, as he is not an experimental scientist but a coal-face GP). In his latest he has returned to the topic he has been hammering relentlessly away at for years: the cause(s) of cardiovascular disease. It looks as though the very first step to take is to make sure you get plenty of Vitamin C.
I am not trying to provoke a fight between Dr No and Dr Kendrick when I say that they are far and away my favourite sources of medical information. Both are well-informed and balanced; both write extremely well and with a welcome touch of humour; and both encourage free and open discussion in their comments sections.
Shawn, Tom and Carolyn – Dr No has always been a little troubled by that passage from Dr K, though this is the first time he has gone public about it (even Dr No worries every now and then about setting off hydrogen bombs in his own back yard). The thing is, it is actually quite rare for a doctor, especially a GP (Dr K did say in June this year that he was a “GP working mainly with elderly patients in Care Homes and Intermediate Care” which implies sessional work, not at all uncommon for GPs who have other interests eg writing and, in Dr No’s case, being a sailing instructor), to be present at the moment of death. Think about it: we would have to have an uncanny knack of being here there and everywhere always at a particular moment in time. This is not to attack Dr K, nor the many excellent posts he has written, but it is to wonder about that ‘After reading this…’ paragraph. Dr No couldn’t help wondering if Dr K had watched too many replays of the Wuhan videos showing people dropping down dead in the streets. It all conjures up covid-19 being a thunderbolt disease, which it is most assuredly not.
Dr No by the way is retired – not seen a patient for years. But that doesn’t mean he no longer thinks like a doctor. Learning to doctor is like learning to swim, once learnt, never forgotten. Especially when thrown in at the deep end. Nonetheless, over the 18 months or so of the pandemic, he has not personally heard of one person who has been hospitalised because of covid, let alone died from it. Only very rarely does he even hear someone say they have had covid, and they say it in the way that someone might talk of flu they had last winter, a nuisance at the time, but that is as far as it went. There is a big reality disconnect between the MSM/official narrative, and Dr No’s (and his friend’s) experience of covid. That will remain the case, even if Dr No catches lab confirmed covid, and subsequently dies.
Shawn – absolutely agree on clinical diagnosis of common or garden covid, ie without all the tests that come with hospital/ICU admission. There are no distinguishing clinical features. Cough, fever and loss of sense of smell – a host of mainly upper respiratory tract illnesses do that. Maybe a history of chronic obstructive pulmonary disease in an older patient, gets a cold or whatever, develops pneumonia, maybe dies, this pattern is as old as the hills, and traditionally we never really bothered about what exactly the ‘cold or whatever’ was, because it was viral, and not a lot we could do, except provide symptomatic care and treatment, in the hope the patient didn’t get pneumonia. Then, out of the blue, came covid, and the covid PCR test, and, by God, how things have changed.
I would say, in support of Dr K that, now I cast my mind right back to March last year I did see a clutch of extremely frail nursing home patients who followed that same clinical pattern that he describes: one where they look well but their numbers were shockingly unwell and there was clearly something going on that was unlike any known illness at that time. But that was then, I don’t believe that can happen now because everyone must now have been exposed to the virus and survived through one mechanism or other.
Shawn – wasn’t having a pop at Dr K, just asking questions about the evidence. Also worth bearing in mind things back in March last year were pretty frantic, with high alert levels, perfect breeding ground for hot stuff bias. If there was a rapidly fatal syndrome cause by covid, there would have to have a remarkably rapid all consuming and widespread burning of dry tinder for the effect to disappear as quickly as it arrived. If, on the other hand, it is the general modus operandi of covid in those it kills, we should have seen it (NAD > sats through the floor > RIP) persist.
And there is this:
“Ten Fatal Errors: Scientists Attack Paper That Established Global PCR Driven Lockdown”
https://uncoverdc.com/2020/12/03/ten-fatal-errors-scientists-attack-paper-that-established-global-pcr-driven-lockdown/
The Corman-Drosten paper detailing the protocol to be used in diagnosing SARS-CoV-2 infection by PCR was published on 23rd January 2020; the submission date and acceptance date of this paper are January 21st and January 22nd, respectively. Apparently peer review of this critically important paper was done within a day or two! Pretty quick work, in the absence of a sample of the virus and with only the supposed sequence provided by the Chinese a couple of weeks before…
While listening to an interview with Dr Wolfgang Wodarg https://rumble.com/vnwzlh-wolfgang-wodarg-full-interview-planet-lockdown.html it suddenly occurred to me: what if, as Dr Wodarg hints, the scientists working on gain-of-function in the Wuhan lab (or elsewhere) knew the exact sequence of the virus – because they themselves had created it?
I recommend listening to Dr Wodarg’s interview. He goes on to suggest that when Corman and Drosten created their PCR protocol they designed it to test for small fragments of RNA that they already knew were in already known viruses, such as certain coronaviruses and SARS.
That way, he points out, Corman and Drosten could set up the PCR protocol to give a specified percentage of positive results when used on any population. No new virus would even be needed.
Dr Wodarg does not sound careless, but I could not help noticing that he refers twice to “Mr Drosten”. Drosten, of course, claims to be a medical doctor, but there is doubt about his thesis which apparently cannot be found anywhere.
Dr Wodarg goes on to say that the whole testing business has nothing to do with medicine; it has, he says, to do with criminology.
The image of “holding out a vial to a judge” inevitably conjures up memories of the late lamented General Colin Powell with his vial of “anthrax”.
https://www.paulcraigroberts.org/2021/10/18/colin-powell-was-fully-vaccinated-but-died-of-covid-19-complications/
Oh very well done, Dr No. I followed all of that. The dangers of impenetrable specialism cannot be overstressed. If the scientifically trained struggle to unpick the narratives we are presented with, how can the majority of humanity, primed over decades of TV/Hollywood ‘reality-fiction’, have a hope in hell of discerning what is real and what is not, and especially when they are being terrified out of any powers of critical thinking they might still possess. And on top of that we have the wretched model makers, creating yet other illusory worlds and claiming them real. Meanwhile, the powermasters and their mouthpieces go on endlessly stating lies, illogicalities, contravening human rights as if this is the normal way of things because they now know they can.
Others have pointed out some questions too, including this one “War has broken out in the scientific literature that strikes at the existential core of Covid-19 and its proposed causative virus”.
Funny how a technique to multiply very small bits of DNA has suddenly become a test! I won’t repeat what has already been said, aside from a further question about how many cycles the technique must go through to find what ever it is they are looking for? Doubling on each cycle, the compounding effects are simply massive!
Yes, I’d agree that specialisation will tend to cause gaps in thinking and will stifle ideas and innovation. To anyone with their particular hammer, everything will look like a nail!
This brings up another thought, I’d read or heard somewhere that all health systems suffer with misdiagnosis, a figure of 15% rings a bell. A rather alarming figure, really (no pun intended).
Twice I’ve had to fight the medical profession to get my now departed mum treated on time. In one case, the consultant told me she was glad I was a pain on the rear end, or it would have been very serious.
All those GP’s sending patients to all sorts of specialists who run a multitude of tests. It’s enough to make my unilateral idiopathic tinnitus ring ever louder… I just wish it was in stereo!
Steve – thanks for the link, a useful read. Those who relish their sanity may prefer not to look too closely at how often we doctors get the diagnosis wrong. Depending on the gold standard used (eg post mortems, reviews of notes) the rates do appear alarmingly high, but it is sometimes worth asking how much difference getting to the right diagnosis would have made (medicine is not always a straightforward linear problem). Too right about the need to keep a watchful eye on relatives, and indeed one’s own, medical journey. Dr No always feels the practitioner’s guilt on this: as a doctor, he knows how to pull levers to open doors in the NHS, but what about others who lack that knowledge?
An excellent article on a subject I have been trying to make sense of since this whole, dare I say it, charade began. On the one hand we have numerous virologists telling us Sars Cov 2 has been isolated and on the other, many intelligent experts saying it hasn’t. One of the main complaints, as Dr No rightly says, is that there has been no control group, with the inference that it was the very constituents of the culture that led to the cytopathic effect when the “infected” material was added to the mix. So, if I read it correctly, it appears Dr No’s analysis of the two studies firmly puts this objection to rest. ie confirmation that the cytopathic effect is only observed when the infected material is added to the mix. However, it would interesting to hear what Stefan Lanka’s view would be on this, as I understand he says he has replicated these procedures and produced a similar cytopathic storm when adding a non toxic yeast rna to the mix. So unless I have misinterpreted the control, I guess that still leaves a slight question re a control group, namely would the same cytopathic effect be observed if the above studies added similar non infected material, rather than nothing at all ?
http://odysee.com/@OurFreeSociety:2/CPE—Control-Experiment—21-April-2021—English-version:0
However, regardless of the above debate, it still seems clear that the “virus” is only ever seen in culture and as far I am aware has never actually been purified or isolated and viewed as an entity on it’s own.
Indeed I seem to recall Dr Judy Mikovits saying in a recent discussion with Dr Andy Kauffman that the virus could not be separated from the cell as it required the cell to provide it’s lipid coating.
So I am left with two burning questions:-
1) If the virus cannot exist without the cell, how is it propagated as we are led to believe, ie as minute aerosolised particles. Are we humans breathing out cells with a virus attached ? I doubt it.
2) If the virus can exist independently of the cell and is allegedly as prolific as we are led to believe, why can’t it be purified and isolated as an entity in it’s own right. Surely it’s still only a molecule, or number of molecules. I believe smaller particles have indeed been purified and isolated so what is special about a “virus” I wonder ?
Maybe because I’m not a virologist I just don’t have a proper understanding of the subject but if anyone can enlighten me on the above I would be pleased to hear
Brilliant work Dr no. You have done all that work so I don’t have to.
One caveat to the praise though. Convinced by the mask wearing advice from on high, I have used mine (now 18 months old) to catch viral particles. My mask is a cut down butterfly net, designed to catch but not harm the virus. I must have at least a thousand viral particles, but they are too small to see. Would you like me to send you a couple?
PS seriously, that article is a truly great piece of work, thanks +++
Hang on a mo’, doc. Is it really the case that the whole shemozzle is based on only two decent papers? Just two?
dearieme – no, Dr No just picked two seminal early papers, that still influence the current official understanding of the virus. A comment coming up shortly on some other observations (or rather, the striking absence of observations…).
Does your analysis affect your views on the advisability of taking the jab, doc? Especially the booster jab?
dearieme – tricky to answer, because it sails very close to the wind on giving personal medical advice online. Doctors who do genuinely and in good faith believe in the vaccines could get very upset if Dr No started advising (individual) patients on what to do. What he can say, because by definition it is in the public domain, is that there is a lot of information out there, and any wise patient who wants to make sure they give informed consent will naturally want to read up on things before coming to a decision.
Dr No has tried to come up with a jobbing doctor’s analogy for how viral diseases replicate and spread. Let us imagine viruses are like chain letters. Once in a house, they replicate, and get sent out again, where they travel as inert letters to the next house which they infect, and so can replicate again, before getting sent out again as inert objects that will go on to infect other houses. This analogy works better than a computer virus, because we can see the physical letter’s envelope as the virus’s outer containing layer, and the letter itself with the instructions on how to propagate the chain as the DNA/RNA in the virus. Dr No the jobbing doctor always assumed those letters were analogous to the viral particles that get spread by aerosols, with some hanging around on surfaces for a while.
So far, so good. Next up, a google image search for photos of a virus (any virus, not just covid) on a surface (any surface). After all we all have very clear images in our heads of what viruses look like. Dr No expected tens of thousands of hits, and he certainly got plenty of hits, but not one of a single virus on a surface. Cripes. Dr No appreciates you need a bit more than an Instamatic to snap a virus in the wild, but not one photo? There are plenty of photos of viruses in culture and/or on/in cells, as in the photos in the post, but that’s it. It seems all the covi-serfs are diligently disinfecting surfaces for something that has never been seen. The Milk Curdler’s Multiphase Turbulent Gas Clouds are blown away! Macavity the mystery virus strikes again! Out in the wild, Macavity’s not there!
There are some images of viruses on what look like some sort of surface in some scientific papers, eg vaccinia (related to smallpox) and Ebola here, but none of them – at least those Dr No has come across – say what the background is. These images (in the link) are scanning electron micrographs, which have a 3D appearance, and transmission electron micrographs, which are 2D, and look more like conventional light microscopy slides. Note that all electron micrographs are black and white: any hint of colour means at least some Photoshopping has been applied. The 3D effect in scanning electron micrographs is also somewhat limited in depth of field, and cannot achieve perspective effects, something worth bearing in mind when trying to decide whether an image is real world, or computer generated, which an awful lot are.
Peter’s question (2) above does appear to raise some very interesting questions.
Dr No’s mention of “hell-broths” reminded me of the following, which made my hair stand on end when I first read it a year or so ago. True, it’s about vaccines rather than viruses, but I think the idea is similar.
“I think one of the major problems with vaccines is that they’re grown in animal tissues and we don’t know what viruses and pathogens are coming back in the needle. A recent inquiry in December 2018 by the Italian lab, Corvela, on the GlaxoSmithKline vaccine Priorix Terta highlights troubling problems that our technology can now uncover but that few seem to have the courage to investigate. Translated from the Italian, the report finds:
“We have continued the investigation, both chemical and biological, on the Priox Tetra, quadrivalent against measles, rubella, mumps, and varicella. We have found . . . proteobacteria and nematoda worms, 10 other viruses through ssRNA, Microviridae (bacterial or phage viruses)
and numerous retroviruses including endogenous human and avian retroviruses, avian viruses, human immunodeficiency and immunodeficiency virus of monkeys (fragments that if inserted into the database detect fragments of HIV and SIV), murine virus, horse infectious anemia virus, lymphoproliferative disease virus, Rous sarcoma virus, alphaendornavirus, hepatitis B virus, and yeast virus…
“If you eliminate the animal tissue, that leaves aborted human fetal tissue, and I think there are significant moral and scientific issues with what happens on a genetic level when you inject human tissue into the bloodstream. Then you get to the issue of chemicals in the vaccines, like mercury, aluminum, formaldehyde, polysorbate 80, and a host of others, and it begins to look like a witch’s brew that would only be given to children in some demented fairy tale”.
“PLAGUE OF CORRUPTION
“RESTORING FAITH IN THE PROMISE OF SCIENCE”
Dr Judy Mikovits and Dr Kent Heckenlively
(Amazon Kindle Edition)
On reflection, isn’t it a tremendous testimonial to the power and flexibility of the immune system that people can be injected with stuff like that and NOT die?
In the hope of getting himself proved wrong, Dr No tweeted this earlier today (and re-tweeted it again just now). As you can see, no takers yet:
I remember reading a few articles based on the same suspicions, Dr No. This one, for example:
“How are viruses discovered and identified in the first place?”
https://blog.nomorefakenews.com/2020/02/18/how-are-viruses-discovered-and-identified-in-the-first-place/
Although I am ignorant of science, I like Jon Rapoport’s work – but I must admit I suspect him of being an “enthusiast” who might sometimes get a bit carried away. In this case, however, I can’t find fault with anything he says.
Incidentally, Kary Mullis seems to have been very sceptical – to the point of disbelief – that AIDS is caused by HIV. From online interviews and reading his book, I gather that he was inclined to blame extreme lifestyles, fatigue, drugs, malnutrition and pollution. Significantly for Covid-19, Mullis also speculated that some of the viciously toxic drugs given for AIDS – such as AZT – actually killed a lot of the patients. In Africa and other places lacking sophisticated labs, Mullis thought that anyone seriously ill who couldn’t quickly be diagnosed with a “proper” disease would be categorised as “AIDS”, given the drugs, and – when they died – listed as AIDS deaths.
Hear any echoes yet? People sick with a mysterious ailment who were put on ventilators and then died, listed as Covid-1`9 deaths?
Another excellent article is this (by Torsten Engelbrecht – co-author of the book “Virus Mania” – and Konstantin Demeter):
https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/
Also this, which refutes a “fact check” of the previous article:
https://off-guardian.org/2020/07/31/open-letter-refuting-politifacts-fact-check/
and these:
https://off-guardian.org/2021/01/31/phantom-virus-in-search-of-sars-cov-2/
https://off-guardian.org/2020/11/17/covid19-evidence-of-global-fraud/
https://off-guardian.org/2020/07/02/no-one-has-died-from-the-coronavirus-president-of-the-bulgarian-pathology-association/
among many others.
Just thinking out loud, and I know beware correlation… but the rise in allergies to this and that seems to me to match the rise in vaccination over the last 50 years, particularly in children. Vaccines mess with the immune system, allergic reactions are an over-sensitivity of the immune system.
Allergies are less common in poor Countries where vaccination is at a much lower level. In my earlier life pre-1980s, allergies were so rare I cannot ever remember hearing about them or people dying, apart from wasp or bee stings. Peanuts were widely consumed without reported incident except the occasional unfortunate who choked on one.
As for science: it seems what once was a process of investigation of the probably infinite unknown, has morphed into ‘The Science’ which is the Gospel of Certainty – Unquestionable Assumptions (we cannot think of another explanation) by a clerisy of Experts.
A propos vaccines, their effectiveness and safety, you couldn’t do better than read that hefty and horrifying – but devastatingly well referenced – book “Dissolving Illusions: Disease, Vaccines, and The Forgotten History” by Suzanne Humphries and Roman Bystrianyk.
Every doctor ought to read it – twice – and most patients could benefit too.
‘Looking at the data from the United States starting from 1900, the measles mortality rate had declined by more than 98 percent before the DTP vaccine was introduced! I was stunned that no one I knew, including my sons’ doctors, had carefully examined this fundamental belief that vaccines were responsible for the massive decline in deaths from measles and whooping cough’. [Roman Bystrianyk].
‘That winter [2009], three patients in close succession were wheeled into the emergency room of my hospital with total kidney shutdown. When I arrived to talk to them, each one volunteered to me, “I was fine until I had that vaccine”. All three had normal kidney function at baseline, as per their outpatient records. All three required acute dialysis, two eventually recovered and one died of complications several months later, supposedly from his other illnesses. After this series of events, I began to take vaccine histories on each of my patients and was startled at the connections that could be made just by asking, “When was your last vaccine?” In my opinion, many cases of supposedly idiopathic (a medical term for unknown) kidney disease are not idiopathic at all’. [Suzanne Humphries].
‘Try re-vaccination – It never will hurt you,
For re-vaccination has this one great virtue:
Should it injure or kill you whenever you receive it,
We all stand prepared to refuse to believe it’.
– From a circular signed “The Doctors”, 1876
‘Decorous and admissible language fails me, in alluding to that which might have seemed incredible thirty years ago – the commanding of vaccination on the second child of a family, when vaccination has killed the first; and then sending the father to prison for refusal’.
– Emeritus Professor F.W. Newman (1805-1897), October 26 1874
‘Graph 11.7 shows a huge spike in deaths from diphtheria in Leicester immediately after the diphtheria antitoxin came into use in 1895’.
‘[The 1916 New York polio epidemic was thought to have caused 23,000 cases and 5,000 deaths through new England the Middle Atlantic states. The case fatality rate of 25% was far above the rate for “wild” polio of less than 1%.].
Three miles from the epicentre of the outbreak, Simon Flexner and his associates at the Rockefeller Institute at 63rd Street and York Avenue… had been passaging spinal cord tissue containing poliovirus, from one Rhesus monkey spinal cord to another… It is a remarkable coincidence that a unique neurotropic strain of poliovirus was developed a few miles away from an epidemic caused by a uniquely pathogenic strain of the virus… almost anywhere in new York was within a few streets of a rail link to the Rockefeller Institute’.
[And it’s less than two miles walk to Grand Central Station!]
‘… “the immune system remains a black box,” says Garry Fathman, MD, a professor of immunology and rheumatology and associate director of the Institute for Immunology, Transplantation and Infection…. “Right now we’re still doing the same tests I did when I was a medical student in the late 1960s…” It’s staggeringly complex, comprising at least 15 different interacting cells types that spew dozens of different molecules into the blood to communicate with one another and do battle. Within each of those cells sit tens of thousands of genes whose activity can be altered by age, exercise, infection, vaccination status, diet, stress, you name it… That’s an awful lot of moving parts. And we don’t really know what the vast majority of them do, or should be doing… We can’t even be sure how to tell when the immune system’s not working right, let alone why not, because we don’t have good metrics for what a healthy human immune system looks like. Despite billions spent on immune stimulants in supermarkets and drugstores last year, we don’t know what – if anything – those really do, or what “immune stimulant” even means’.
– B. Goldman, “The Bodyguard: Tapping the Immune System’s Secrets”, Stanford Medicine, Summer 2011.
When I was young “allergies” were sometimes viewed as bogus weaknesses to which somewhat hysterical Americans were prone. But, I suppose, it’s perfectly conceivable that US pollens (for instance) are more of a problem that UK pollens.
I had never suffered from hay fever when living in Scotland and Yorkshire. It started for me when I moved to Cambridgeshire – a common problem according to my GP.
I’ve been thinking this for some time now and I wonder if Dr No, or others, have ever considered the same. Namely, what, if any, the case count might have been if we had carried out the current levels of PCR testing, using the existing methodolgy before the alleged advent of Covid ? The current scientific “concensus” would no doubt have us believe zero but would it be ?
Indeed, is there any way of testing stored bodily samples prior to say October 2019 to prove this one way or another ?
Or if PCR testing were done now for other viruses such as flu?
“But, I suppose, it’s perfectly conceivable that US pollens (for instance) are more of a problem that UK pollens”.
Perhaps human habitation goes back much further in Africa, Europe and Asia than in the new World. Giving our ancestors longer to adapt.
On the News this morning, it has been admitted Track & Trace failed in its primary aim to get life back to normal, but… it played an important party in management of the pandemic. Of course it did… what exactly?
In the matter of testing. We’ve been there before.
‘ In late July, the CDC abruptly advised states to stop testing for H1N1 flu, and stopped counting individual cases,” CBS News reported in 2009. “The rationale given for the CDC guidance to forego testing and tracking individual cases was: why waste resources testing for H1N1 flu when the government has already confirmed there’s an epidemic?”
Why indeed? But then, unlike now, the objective was not to use it to cause widespread fear and panic in order to exercise new-found power to play tyrant.
Full piece here makes interesting reading.
https://www.foxnews.com/politics/flashback-obama-admin-halted-state-h1n1-testing-complicating-bidens-attacks-on-white-house
I’ve been musing about getting a booster jab. I think not, at least not yet. My logic is that the Powers That Be seem to be taking outrageous risks with the lives and health of children and adolescents, so why should I imagine that they aren’t planning to take outrageous risks with mine?
Falsus in uno, falsus in omnibus.
dearieme – thank you for your candid disclosure, others will no doubt appreciate it, and ponder it, as they ponder their own decisions.
The ‘are viruses for real’ question won’t go away, so Dr No had done another post, Schrödinger’s Virus, looking at the crucial purification step in getting from a hell broth to a single viral cause of disease. It turns out naked virus has been photographed in the wild, at least for polio, but that is about as good as it gets. The rest remains as murky as a hell broth must.