
Still Dropping Like Flies
Earlier this week the GMC at long last released data on the number of doctors who died while undergoing fitness to practice investigation and monitoring. The number of deaths should be extremely small — the individuals at risk are working age adults with good socioeconomic status — and the numbers are small, on average about ten a year in recent years. But are these numbers really that small? For comparison, there are currently around twenty deaths in police custody annually in all England and Wales, a conceptually similar but in other respects very different so-called never event that should never happen. When Dr No last wrote about what we might loosely call deaths in GMC custody, in 2013, the annual number of deaths, revealed after a FOI request, was very similar, around eleven, a number subsequently confirmed in a 2014 internal GMC review, which also revealed that around one in four of the deaths were suicides. In the data released this week, around one in five or six of the deaths were suicides.
The high proportion of suicides sent a signal that the harshness of the GMC’s long drawn out processes, which are notoriously punitive, obnoxious, adversarial and Kafkaesque, might be partly to blame for the deaths. The GMC duly did some public hand-wringing and bed-wetting, and promised to clean up its act. And yet here we are, almost a decade later, and the annual number of deaths is pretty much unchanged, though the proportion of suicides may perhaps be slightly less. On the face of it, the GMC’s claim that it has made its processes more humane appears not to be borne out by the figures — the never events are still happening at the same annual rate. But, as ever, the devil is in the detail, in this case the number of individuals at risk. If, for example, the annual number of doctors investigated by the GMC has doubled, and nothing else changed, then we might expect the number of deaths to double. We need to determine how many doctors underwent fitness to practice investigation a decade ago, and how many are subject to investigation these days. We can then compare rates, to determine whether things are getting better or worse. We can also, albeit very crudely, compare the number of deaths we might expect in a similar population not undergoing fitness to practice investigation to the observed number, and determine whether our doctors are indeed dropping like flies, or dying pretty much at the rate we would expect.
The denominator, the number of doctors at risk, is surprisingly difficult to determine. Not only do the number of doctors reported to the GMC vary year on year, changes in the way the GMC handles complaints have also changed over time, meaning considerable variations in the number of doctors who end up under investigation. And then there is the question of when does an enquiry become an investigation? If there is a preliminary enquiry, as there often is, does that amount to being under investigation, or is that stage only reached when the GMC commits to a full investigation? And finally, there is the duration of the investigation. The GMC is notorious for the bovine slowness of its processes, which can take years to conclude. A doctor whose investigation starts in one year may well still be under investigation over a year later, and so is still part of the at risk population, but will only be counted once, in the year the in which the investigation started.
The GMC now has, like every other organisation you would rather not know about, a dashboard which has a chart showing the annual number of investigations since 2007. These are so called full investigations, which by and large happen when the doctor faces allegations that could put his or her registration at risk. The chart shows that, apart from a sharp peak in and around 2013, the number of full investigations was similar in the late noughties to that seen in more recent years. However, the average annual number of full investigations for the period 2007 to 2013, which overlies the 2005 to 2013 period covered in the GMC’s 2014 report, is 2,105, compared to 1,404 in the period covered by the GMC’s latest 2018 to 2020 figures. This means annual crude mortality — average annual deaths divided by annual number of new investigations — has marginally increased, not decreased, in recent years, from 6 per 1,000 to 7 per 1,000. The crude confirmed suicide rate has remained pretty much the same, at a little over 1 per 1,000, though the actual rate is likely to higher, because not all suicides end up as confirmed suicides.
These rates come with all the usual caveats. The annual numbers of events (deaths) are extremely small, there are classification problems (when does a doctor become ‘at risk’, how many suicides are not recorded as suicides), The duration of fitness to practice investigations may also have changed over time, thus increasing the number of person-years at risk, but that does not appear to be the case. For the period 2013 to 2020 (the only period for which Dr No has been able to find comparable data), the total number of cases still open after one year varied from 477 in 2015/16, to 919 in 2013/14 (and was 800 in 2019/20), while the median time in weeks from initial complaint to final hearing ranged from 80 in 2018/19 to 107 in 2016/17. By and large, although there is considerable year on year variation, it appears GMC investigations still take an unacceptably long time to reach conclusion.
There remains one other problem in the denominator in the GMC’s latest report. The total three year number of full investigations in this week’s report appears to agree with the dashboard (around 382 of the preliminary enquiries became full investigations, which if added to the 3,834 always full investigations gives a total of 4,216, compared to 4,213 from the dashboard), but the report then obfuscates things by breaking down the deaths into deaths while under investigation (n=19) and while being monitored (n=10). This appears to be a lump of mud thrown in to muddy the waters, but there is a way round it. Any doctor being monitored has also been under investigation. He, or more rarely she, has just had the double hit of being investigated and monitored. We can keep the denominators as they are, and just bear in mind that the doctors being monitored will very likely have had extended periods of exposure to GMC duress.
Finally, and perhaps most importantly, how do these numbers of deaths compare to the number of deaths we might expect in a similar population not subject to GMC investigation? But what reference population to use? Annual working age specific mortality rates can be calculated readily enough from standard ONS data for all individuals (very roughly, 3/1000 for men, 2/1000 for women), but that is not much use, given the wide range of mortality experienced by different socioeconomic groups. Age standardised mortality rates are available for many professions, including health professionals, whoever they are, but those rates (2.25/1000 for men, 2.13/1000 for women) include all ages. What we need is the intersection of these two rates: what is the mortality rates in working age health professionals? Unfortunately, the data is not available, and so we are going to have to use a proxy. Proxies always carry a statistical health warning, but we do have the above all working age and all health professional rates as sanity checks.
The closest proxy Dr No has found is a study that reports age and sex specific mortality not by occupation or socioeconomic group, but by geography and deprivation, for 2017. The research is up to date and thorough, and contains age band and sex specific mortality rates by deprivation, from the most deprived area to the least deprived. To allow us to use the mortality rates in this study as a proxy, we are going to assume that the mortality of doctors is broadly in line with the mortality rates found in areas of low deprivation, regardless of where the doctor actually lives. Dr No does not think this is an entirely unreasonable assumption: a doctor, wherever he or she lives, will enjoy many of the health benefits available to those who do live in the affluent areas, notably high income and generally healthy lifestyles. Turning to Figure 2 in the study, we can eye-ball the right hand ends (the areas of least deprivation) of the orange (2017) lines, for males and females aged 40 – 54 — see the screen grab below — (and perhaps the charts for ages 25 – 39 and 55 – 64; note the captions for individual charts are above, not below, the charts) and come to mortality estimates of 1.75 per 1,000 for males, and 1.6 per 1,000 for females for these affluent areas. These figures are not exact, but neither do they fall foul of the sanity checks above: they are, Dr No suggests, good enough.
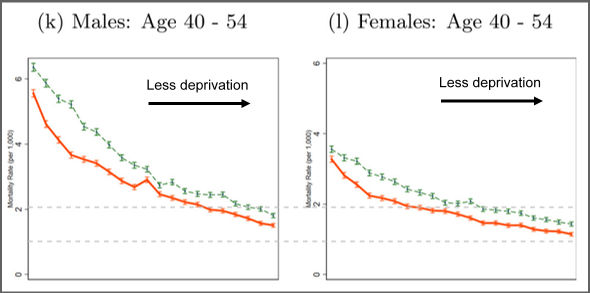
Screengrab 1: Death Rates (Deaths per 1,000 population) for 40 – 54 year olds, by ventile of deprivation and sex in 2003 and 2017. Note the very sharp gradient moving left to right, from the most deprived areas to the least deprived. Source: see text
The GMC dashboard shows visually (unfortunately, the data download option doesn’t work…) that around three quarters of those investigated are male, and the majority are middle working aged (which is why Dr No used the 40 -54 year old charts, noting that the ones on either side probably cancel each other out). Of the 4,200 doctors under investigation over the recent three year period, around three quarters, or 3150, are male, and 1,050 are female, giving an expected number of male deaths of 5.51 (3.15 x 1.75 = 5.51) and an expected number of female deaths of 1.68 (1.05 x 1.6 = 1.68), making the three year total number of expected deaths in age/sex matched peers from a similar socioeconomic background but not undergoing fitness to practice investigation a grand total of 7 (5.51 + 1.68 = 7.19, rounded to 7). Among the doctors undergoing fitness to practice investigation, that number was 29, making their mortality rate compared to those enjoying similar life experience, but without the weight of a GMC investigation on their back, four times higher.
Dr No has taken pains to underline the fact these findings rely on a proxy measure, and there may be other confounding factors, not least the possibility that the doctor under investigation came to the GMC’s attention because he or she was ill, and so was already at higher risk of death, though in a sane humane world these doctors would be managed and indeed cared for well away from the GMC, and never come near its fitness to practice procedures. Nonetheless, on the basis of the data and results presented here, which rely on a methodology that Dr No considers is an improvement on the method he used in 2013, we find there is a fourfold increase in mortality among doctors under GMC investigation, compared to comparable individuals not undergoing investigation.
A decade ago, Dr No characterised the mortality of doctors dying while under GMC investigation as ‘dropping like flies’. Ten years on, after a lengthy period in which the GMC has been at pains to say it has made its fitness to practice processes more humane, we find that little has changed. Doctors under those processes are still dropping like flies.
Kendrick’s recent post made the GMC sound like a conclave of Witchfinders General.
https://drmalcolmkendrick.org/2022/02/27/vaccination-silencing-doctors-in-the-uk/
The crime alleged in the tale he tells is about a doctor who “questioned some aspects of the safety and efficacy of the vaccines”. That’s it – he didn’t grope women, saw off the wrong leg while drunk, or commit any of the other offences for which the medical trade has a lurid reputation.
Oh well, we must strain every sinew to persuade the world of the ineffable superiority of the habits of our liberal democracy, eh?
Dr No saw that Dr Kendrick post, and added a few comments, including a remark that it was GMC behaviour that started Dr No blogging way back in 2009. The GMC has a history in recent decades of behaving like Witchfinders, but way back ie when Dr No first walked the wards, the Blue Book (the code of conduct) was wafer thin, and the closest most doctors ever got to the GMC was sending it a cheque to cover the annual retention fee.
There are lies, damed lies and statistics aren’t there? This article makes it very clear that the GMC is being judged as performing poorly and acting unreasonably, providing a point to be proven. I am interested in knowing how the death rate of doctors compares with that of other professionals being investigated by their professional bodies? And how much investigation has there been into other factors that might explain why some under investigation choose suicide while others do not, such as autistic traits which multiply your risk 10 fold. To what extent to doctors rely on their professional status for their sense of identity and social status compared with other occupations? Maybe the GMC does need to reform how it investigates complaints against doctors but the arguments in this article are pure smoke and mirrors
The GMC has historically tended to be coy about deaths while an individual is under investigation, for obvious reasons. The GMC only released the data in 2013 in response to a FOI request, and then did the Internal Review in 2014, and have only now committed to releasing the data on an ongoing basis. It should at least be commended for doing that. Dr No has not looked at what other regulators have done, but he would not be surprised if they too tend to be coy.
The 2014 Internal review (link in first paragraph of post) has a lot of data in it on those who died by suicide, including concurrent mental illness. In a humane system, these ill doctors should almost invariably not be anywhere near the GMC’s fitness to practice procedures. They are, to use psychiatric parlance, not bad, but mad or sad.
Doctors’ own sense of identity and self is very often tied up with their profession status, making them vulnerable when that status us attacked. No doubt the same applies to other professions, particularly vocational professions, where the same links between identity, self and profession apply.
As for smoke and mirrors, well, Dr No apologises! He does his best to be clear…
Nothing will change until MPs are subject to a similar procedure.
Talking of doctors and regulation, what on earth am I to make of this strange tale?
https://www.theguardian.com/uk-news/2022/mar/06/nhs-surgeon-censured-for-vandalising-colleagues-cars
For doctors, all cautions and convictions have to be reported to the GMC, which then decides whether it needs to take action. This surgeon was then found guilty of bringing the profession into disrepute, which does seem a little OTT. How does a doctor in London get brought into disrepute by a surgeon having a tantrum in Leicester? The problem is that the GMC has increasingly taken a view that extra-curricular activities have professional implications, giving it new ways of being Kafkaesque. You will note from the article there was no question mark over the doctor’s surgical practice, rather the opposite in fact.
“Among the doctors undergoing fitness to practice investigation, that number was 29, making their mortality rate compared to those enjoying similar life experience, but with the weight of a GMC investigation on their back, four times higher”.
With my “editor” hat on, should “with the weight” read “without the weight”?
Tom – well spotted, as ever, thanks. Corrected.
“How does a doctor in London get brought into disrepute by a surgeon having a tantrum in Leicester?”
It must have been about 25 years ago that I noticed people using the word “professional” to mean something like ‘wears respectable clothes and sports a respectable haircut’. In those terms keying cars would undoubtedly be ‘unprofessional’. What silly buggers we’ve all become – excluding thee and me, presumably, doc.
P.S. Moreover, this GMC lark presumably inhibits the proper treatment of the tantrum kid i.e. a posse of the injured should give him good hiding.
The number of deaths of doctors who are subject to the Kafkaesque processes (or process failures) of the GMC is but the tip of the iceberg. It would be instructive to look at wider effects on those doctors and effects on their nearest and dearest. I am old enough to have known several doctors who have been through the GMC investigation mill. None of them were eventually found ‘guilty’ of misconduct despite up to 3 years of being sucked into the rabbit-hole where complainants (sometimes colleagues, not just patients) received no scrutiny and retired old buffers are called as expert witnesses to pronounce on matters wholly outside their expertise. All these people had spouses who, like the accused, spent 2 or 3 years without a full night’s sleep. One of them had a daughter who later committed suicide and I have always wondered how much her father’s experience (trusted GP in a small market town, pillar of the community so the GMC case was highly visible) affected her.
It is not just fear of losing livelihood and identity. It is also the fear of being splashed all over the tabloids and total bemusement at how a professional regulator can be so thoroughly unprofessional to the point that they often commit sins far worse than those the doctor is being accused of.
Hippocritical – thank you for making the important point about the deaths being the tip of an iceberg of misery. Dr No has so far escaped the clutches of the Inquisition or perhaps more accurately the Stasi, but he too has had friends who have not been so lucky. It was after all the constructive erasure of an at times eccentric but well meaning friend from medical school days that became a major stimulus that led Dr No to start blogging back in 2009.
Doctors get investigated for not mowing the lawn, for affairs, for parking tickets. In my latest case, for enquiring for a non-doctor job trying to leave the profession whilst still trying to help in the pandemic as the ****** GMC will not allow me to actually work as a doctor.
This is quite clearly the tip of the iceburg as suicide is not a vogue cause of death and even wen this occurs, especially if abroad it doe snot state the reason for suicide so the GMC will not count it and say it cannot find reasonably that the doctor dies of suicide attributable to them so needs no further investigation.
The various processes the GMC use are not fit for purpose and often attack doctors personally and systematically with prolong death with a thousand cuts, suicide is a clear easy and stress relieving way out of the situation. Prior to my GMC difficulties I highlighted how the local deanery has used GMC processes to create a local anti-whistleblowing policy as it is effective – this was used to tangentially attack doctors whom raised or could raise concerns about certain doctors/surgeons some of which are in prison and the GMC is unwilling to take any further action given their race.
Having multiple GMC investigations over many years, it is clear the Performance assessment and Health assessment are designed to push suicide, s is the impossible Kafesque term of ‘insight’ used by the GMC https://www.whatdotheyknow.com/request/gmc_insight which the GMC will do everything possible to continue to attack doctors individually and make sure they do not start talking to one another, which has parallels with evolving hospital MHPS or event he GMC banning freedom of speech when under its one-sided investigations.
For anyone who is new to this: The more you speak the more you stand out. However there is an alternative point, close to suicide that speaking out can no longer cause any more problems.
https://www.cambridge-news.co.uk/news/cambridge-news/healthy-cambs-teenager-rushed-hospital-23972514
Is anyone ever going to count the vaccine casualties, doc?
By coincidence ONS discretely released the latest set (to 31 Mar 2022) of all cause, covid and non-covid deaths by vaccination status data last week. If it was complicated before, it is now even more complicated! At some point, Dr No will see if he can make any sense of it. The data, for anyone who wants to have a look, is here.
Morbidity as opposed to mortality is always going to be harder to pin down, given so many have now been jabbed (wiping out a reasonable control group). In due course we will perhaps, only perhaps, see (or not see) increases in the incidence of certain conditions, and may or may not be able to link them to vaccination status.
It appears monkey pox may soon be the new covid. Dr No smells monkey business afoot, and suggests wise punters will see no pox, hear no pox and speak no pox…
Announcement.
I’ve been pondering “Long Covid” while considering the long term dangers of the spike protein released by the jabs. I suggest we use “Long Vaxx” for the long term bad consequences of the jab.
There’s no danger of confusing it with long term good consequences of the jab: it seems now to be universally admitted that there aren’t any.
Since this blog seems to be on sabbatical (and why not?) I hope Dr No will not mind if I contribute this (seen this morning):
https://stevekirsch.substack.com/p/this-one-graph-tells-you-everything?utm_source=substack&utm_medium=email
The ranter who writes The Market Ticker blog draws this to my attention. Golly.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8647674/
Here’s another mode of dying like flies.
https://stevekirsch.substack.com/p/doctors-in-canada-are-dying-at-a
dearieme and tom – all interesting links. Dr No has indeed been on a sabbatical, but every now and then tunes into the old wavelengths to hear what is going on. One noticeable thing, in keeping with the above links, is that there has been evident excess mortality throughout the last year, apart from the first few months of this year, that can’t be attributed to covid, as the numbers of deaths due to covid (by the ONS definition, it’s in Part 1 of the death certificate) are generally far too small. Here’s a plot done about a month ago showing the excess deaths over the last year compared to the 2015-2019 average (incorporating some covid periods, as ONS does, makes no sense). The plot also reverses ONS’s trick of putting covid deaths at the top of the bars, to make it look like covid is causing (some of) the excess deaths, and instead puts them at the bottom, where they appear as part on the normal, expected mortality. The numbers in the plot are also due to covid, not involving covid. The left hand side of the plot is the second half of 2021, the right hand side the first half of 2022:
At some point, Dr No may get round to looking more closely at what might be causing those excess deaths. At the moment, the available data isn’t detailed enough, only a very limited breakdown by cause of deaths, and the monthly deaths data only includes the top ten leading causes of death, which still isn’t really detailed enough.
Thanks, Dr No! Much appreciated, and very good to hear from you again.
The Old England Journal of Medicine reports a case that may be relevant to your post, doc.
https://www.dailymail.co.uk/health/article-11204547/Why-medical-regulator-pursuing-one-worlds-leading-cancer-specialists.html
Aw, for God’s sake, doc. My wife had an appointment at the hospital today: the silly buggers were insisting patients wear face masks. Are the medical staff all illiterate?
It would be just as effective to erect a totem pole in the entrance way.
Some have got rid of the totem poles altogether. There was an interesting development a few days ago: Air Canada announced it was ending all compulsory covid restrictions because, to quote the press release, “the measures were not justified by science”. Unsurprisingly the coviderati have been in full hue and cry ever since, with some claiming it was fake news. But it wasn’t: Dr No has satisfied himself the press release is genuine. Here is a screen grab:
The web page is still live, and can be seen here. In case it disappears, the Wayback Machine already has an archive copy here.
If it is a hoax, it is a very good hoax that has fooled even Dr No.