
Lies Damned Lies and Best Endeavours
In its efforts to create a troubling and gruesome public opinion atmosphere over covid, the government of People’s Republic of Great Britain have never felt in the least bit shy about inflating the numbers to serve its purposes. Dr No, and a good many other observers, have consistently pointed out the artifice of relying meaningless positive PCR tests to define cases, and of allowing covid to trump the natural underlying cause of death on death certificates. Both conveniently inflate the numbers, such that we might observe that the authorities look at a covid number in the same way that a party organiser looks at a balloon, as something to be inflated. Given flagrant inflation of two of the three main covid numbers, cases and deaths, might it also be the case that the third number, hospitalisations, is also inflated?
Numbers on hospitalisations by cause are notoriously unreliable. They rely on both the doctor putting the right diagnosis in the notes, and the coding clerks extracting the right data from the notes, and both processes are far from perfect. Errors are far from rare, as can be seen here, and these are only identified, albeit corrected, errors. Coding rules and criteria change from time to time, and so it is not in the least bit surprising that difference reports on daily hospitalisation numbers vary, despite claiming to represent the same thing. Add in the complexities of ways of defining covid admissions — usually a recent or in hospital PCR test, so subject to all the regular PCR test shenanigans — and the result is a right royal porridge of numbers that just gets thicker the more you stir it. With these caveats in mind, what can we nonetheless find out about covid admissions?
Until now, Dr No has only looked at admission numbers, suspecting that they were inflated — if only because patients are more likely to get a covid test than have a hot lunch in hospital these days — but unable to find any evidence that this is the case. Then by good fortune he noticed this week a supplementary report, buried at the bottom of the NHS’s Covid–19 Hospital Activity page. It contains, from late June 2021, daily numbers of beds occupied by all patients with covid–19 and, in a separate table, those who had a primary diagnosis of covid–19. Bingo! It’s not admissions, it’s bums in beds, but that’s good enough. By simple subtraction we can plot those who were in hospital with covid as the primary diagnosis, and those who were in hospital for some other reason, who just happened to have covid at the same time. Figure 1 shows the results.
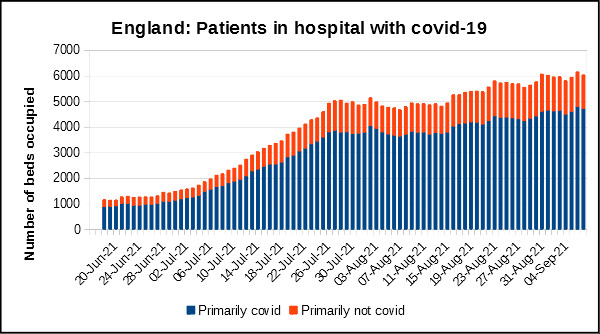
Figure 1: the daily number of beds occupied in England by patients ‘with’ covid–19
The preamble before the link to the supplementary report contains some mellifluous waffle about not putting too much stock in the numbers, on account of the fact trusts only assemble the data on a ‘best endeavours’ basis. Nonetheless, best endeavours notwithstanding, the chart shows that around 20% of patients in hospital ‘with’ covid are not in hospital ‘for’ covid; or to put it in inflationary terms, the numbers with a primary diagnosis of covid–19 have been inflated by 25% or so to generate what the NHS calls the ‘headline published numbers [which] to date have been “inpatients with confirmed Covid” without differentiating between those in hospital “for” Covid and those in hospital “with” Covid’. The headline numbers are inflated, by including patients with coincidental covid, in hospital for a non-covid reason.
It is now clear that all three of the three main measures of covid–19 activity — ‘cases’ (quotes, because they are actually test positives, not cases), admissions and deaths — are all inflated; and, as Dr No’s esteemed colleague Goldfinger likes to say, when things happen in threes, the first time is happenstance, the second is coincidence, and the third is enemy action. Make no mistake, the government has been deliberately and systematically using its ‘best endeavours’ to inflate covid–19 numbers, the better to cower people into submission. Dr No’s advice? Don’t be fooled by this mendacious chicanery.
Thanks, Dr No, for yet another informative and amusing article. I must admit that, glancing at the graph before scrolling down to see the legend, I fervently hoped that it was the blue bars that were the “primarily not covid” figures. Oh well, you take what you can get… and anyway it’s all made up. How many of those people in hospital had flu, for instance? (Since flu has been missing in action for a long time now. I gather that Australia has not recorded a single flu death since July 2020).
Your very well-taken point about the unreliability of official data reminds me of some mild criticism directed at Dr Ioannidis’ latest paper https://www.tabletmag.com/sections/science/articles/pandemic-science, over at Dr Kendrick’s blog. https://drmalcolmkendrick.org/2021/09/03/i-have-not-been-silenced/#comment-233225
I, too, was struck when reading the paper by Dr Ioannidis’ very conservative attitude – he seems to accepty a number of official statements and numbers that I very gravely doubt. But what is an honest epidemiologist to do? (Certainly not to play with his computer and issue terrifying threats of global disaster supported by no actual evidence). Epidemiologists, as I understand it, rely almost wholly on the numbers that other people supply them with. If the numbers are bent or altogether untrue, I don’t see much that the epidemiologist can do without becoming a polemicist. (Which, of course, is our job not his).
Lastly, where are those mendacious chickens to be found? Are they the ones that are coming home to roost in Whitehall and Downing Street? I sincerely hope so.
This morning the Daily Sceptic (Lockdown Sceptics as was) published this admirable cartoon.
https://dailysceptic.org/wp-content/uploads/2021/09/follow-the-science-1.jpg
I do love a good cartoon. Sometimes they actually present the truth better than any number of words could, simply because it hits you in one instantaneous blast.
“But what is an honest epidemiologist to do?” Are you discussing a null set?
When I was a mathematical modeller if I had a poor opinion of the data available to me I would set up an experiment and measure them myself. Them wuz the days. Don’t you just miss science?
As for the epidemiologists – the “maths” they do is so trivial that I wonder how they fill their days.
Maybe rubbing crystal balls is more time-consuming than I would have guessed. Or perhaps they are trying to master the spelling of “charlatan”.
I fear you may be throwing out the baby with the bath water.
“Dr Ferguson is an epidemiologist”. (Actually he isn’t, but let it pass for now).
“Dr Ferguson is an industrial-scale liar”.
Does this logically imply that “All epidemiologists are liars”?
No.
An interesting essay from Ioannidis, though rather circumlocutory for Dr No’s taste. One has a sense of all the right words, but not necessarily in the right order.
Hearing Fergie being promoted to vaccine expert on the Today programme this morning, Dr No had to wonder why on earth a discredited numerological fantasist was being given such airtime on the BBC’s flagship news programme… For those who missed the broadcast, the BBC has coverage here, and the Guardian has the story here. Ioannidis’s essay gives some insight into how this nonsense happens.
Meanwhile, twitter is plugging “Health experts and statisticians explain how fully vaccinated people can test positive for COVID-19” Their’s is a mad desperate world. They might just as well explain how all pigs can be fully fed, and yet some can still fly backwards.
Traditional epidemiology is concerned with the data. Or rather, the data, the whole data (eg getting the right data, minimising bias), and nothing but the data (eg dealing with confounders). Its aim is to describe, often using mathematical terms, the observed world, and it follows that all epidemiology only ever concerns the past. The problems begin the moment ‘epidemiologists’ – ie the numerological fantasists – start projecting beyond the data, and into the future. This is not epidemiology (the study of epidemics, and you can only study something that has already happened), but merely the use of calculators of varying complexity to ask ‘what if’. The underlying fatal flaw is that it uses extrapolation – it goes beyond the data – into a land where not even the laws of gravity apply, because it is a fantasy ‘what if’ world. It doesn’t exist, certainly hasn’t happened yet, and most likely never will if too much egg has gone into the what if pudding. Fergie is a man with rather too many eggs on his worktop…
Perhaps Dr No got carried away towards the end of the last paragraph. We can put this even more fundamentally. Science studies the natural world, a world which exists, and is (or has been) present, and we can examine. The moment we start to predict the future, which is not yet in the world, because it hasn’t yet happened, we are no longer doing science, because we can’t study something that hasn’t happened. We are instead doing something entirely different, more often than not using algorithms in various guises deployed in various forms of technology to second guess what might happen. We’re laying bets, setting out probabilities, suggesting this might happen, if that happens. The trouble is the modellers rather fancy the kudos of science (so much nicer to be Nicolaus Copernicus with his feet on the ground rather than Mystic Meg pointing at her stars) and so they wilfully blur the boundaries, and encourage us to think the finger pointing at the future is still science. It isn’t, because it is an oxymoron to even suggest you can do science on the future.
You can do science (a process), and you can do predictions (also a process), but to suggest the two are one and the same thing is pure bunkum.
I think Dr No did get rather carried away! What you say is very true in the context of the Covid nonsense, but surely you don’t extend it to the whole of science?
When an aircraft, a missile or a space vehicle is sent up, we trust science when it assures us that they will go more or less where intended.
When a simply computer program to calculate prime numbers is started, we are fairly safe in assuming that it will do so until halted.
Science is based on experiments, and the essence of an experiment is that it correctly predicts what will happen (under very tightly controlled circumstances).
I suggest that it is precisely when we stick very narrowly to science itself that we can safely predict the future. But trying to infer wider consequences can lead to disaster.
As John Kenneth Galbraith remarked,
“There are two kinds of forecasters: those who don’t know and those who don’t know they don’t know”.
Incidentally, although Copernicus did believe the Earth went round the Sun rather than vice versa, he advocated a system with 48 epicycles to ensure that everything in the heavens revolved in perfect circles.
Tom – you are right – Dr No did get carried away, posting before an idea is sufficiently formed.
Perhaps there are three processes, and Dr No hasn’t clarified how he sees the separation between them, especially the last two.
1. Science: the process of observing the natural world, and attempting to understand it. There are two main modes: observation (traditional epidemiology, for example) and experimentation (testing predictions, not widely used in epidemiology for all the usual reasons, but very widely used more generally in medicine).
2. Applied science: the process of applying what we have learnt from the process of doing the science to achieve what we want to achieve in the real world: land a jumbo jet, watch TV, post a comment on a blog. This realm also comes under the heading ‘using technology’: using a combination of what we have learnt from doing the science and some sort of machine to get a desired result.
3. Modelling, forecasting, making what if predictions about the future. The key thing perhaps is this process is abstract. Or maybe it’s the use of extrapolation? But then again, an aeroplane designer working up the plans for a plane twice as large as any that has flown before is extrapolating, because no such plane has ever flown before.
Perhaps another important dimension is system complexity. Landing a jumbo jet is complex, but the system it operates in is (usually) not complex, just a balanced interaction between gravity and aerodynamics. Predicting the weather, or an epidemic, on the other hand, is to attempt to predict a very complex system with large numbers of variables.
The reason for pointing this up is the blurring of (1) and (3) above, with (3) trying to pretend it is (1). That has been one of the colossal mistakes of managing the pandemic: politicos – the ones who make the decisions – thinking they are getting (1), when most of the time they are getting (3).
Thanks for your elucidation, Dr No. I think we are very much in agreement – certainly about Ferguson.
The cartoon that I linked to earlier is entitled “Follow the Science” – and explains that this is not good advice when “the science” is being controlled by politics.
https://dailysceptic.org/wp-content/uploads/2021/09/follow-the-science-1.jpg
As far as I can ascertain, the whole field of virology is very vague and poorly understood – as is the field of vaccinations and inoculations. The general idea seems sound enough – poke the immune system a bit to get it to sit up and take notice. But the immune system is not a dog; it’s immensely complicated, and I would bet that there is no human being alive who understands it as a whole.
Thus any injections such as are being mandated for billions of people amount to experimental genetic manipulation, which I would think obviously immoral, illegal and extremely dangerous. But apparently there is no shortage of doctors, scientists, politicians and bureaucrats who are perfectly happy to gamble with the lives of millions of strangers as long as there is no comeback and they stand to gain.
happy to gamble with the lives of millions of strangers
True, but then not dishing out the vaccines is a gamble too. Deciding not to act is also an action.
My main point was the those dishing out the “vaccines” profit by it – some of them to the tune of billions. So deciding not to act is probably not to their taste.
Moreover, the vaccines cannot be dished out until they exist. In normal conditions, for very well established and understood reasons, it takes at least ten years to create and test a vaccine.
Why would it suddenly be possible in less than one year?
dearieme – you are perhaps forgetting the paramount importance of primum non nocere. There is also the question of acts of commission vs acts of omission.
Both legally and in every other meaningful sense the vaccines are currently an experimental treatment. This then places an extraordinary emphasis on the importance of informed consent, and from what Dr No has observed and heard, true informed consent is very much the exception, rather than the rule. To foist an experimental treatment on individuals without informed consent, when you have as yet no knowledge of medium or long term side effects of the experimental treatment, does amount to ‘gambl[ing] with the lives of millions of strangers’.
Equally, you are right to say not dishing out the vaccines is a gamble, and that’s the whole point: either acting or not acting is a gamble, because we don’t know. The benefits and risks are not clearly established, even in the short term. The vaccines appears, at least on PHE’s accounts, to reduce hospitalisations and deaths, but paradoxically they increase the chances of infection, or more strictly testing positive, in 40-79 year olds (this is what PHE’s latest vaccine surveillance report shows: the figures they report are rates per 100,000, so that takes care of the denominator problem). The benefits, by the way – 143,000 admissions averted etc – rely on some far from transparent numerology, and cannot yet be considered established fact. A treatment that makes you more likely to test positive, yet less likely to be seriously ill or die? On one level this makes no sense at all…
We are left with an experimental treatment of unclear benefits and harms. As a patient, Dr No would expect nothing less than 100% informed consent. As a doctor, he would fully respect a patient’s affirmative informed consent (and would give the vaccine), but at the same time he would not plug the vaccine; instead, he would tell it like it is: an experimental treatment that may reduce serious illness and death (for an unknown period), but because it is experimental, we don’t know whether or not it causes medium to long term harm. In these marginal circumstances, it if for the individual to decide whether they want the vaccine. It all boils down to one fundamental question, what to do in the face of uncertainty, and the only reasonable answer is to let the individual make an informed decision, based on what matters to them. To plug avidly, even some might say recklessly, a vaccine for which neither the benefits nor the harms have been properly established appears, at least to this doctor, to be at great risk of violating primum non nocere.
Apparently the Minister for Gloop Deployment slipped into the Commons late yesterday to announce the four nations CMO’s have unanimously decided to go ahead with plugging vaccinations for 12-15 year olds. The lap dogs jumped exactly as expected.
On your earlier comment ‘When I was a mathematical modeller if I had a poor opinion of the data available to me I would set up an experiment and measure them myself’: is Dr No right in supposing that the modelling you did was limited to fitting equations to the data, and did not extend to making extended (and so extrapolated, and very possibly wild) predictions based on those equations? Back in the early 1980s, when Dr No qualified, and well in to the 1990s, when he did much of his epidemiology, ‘modelling’ wasn’t really ‘a thing’ in medicine; instead, we fitted equations to the data, to describe the real world as best we could, and in that sense were doing science (as in (1) in the comment above), an entirely different process to making predictions about the future.
The big problem is the blurring of the meaning of ‘modelling’ to cover both descriptive science done on the real world on the one hand, a valid and useful activity, and, on the other hand, making wild predictions about the future, a highly dubious and potentially dangerous pseudo-scientific activity.
Interesting Ngram (note: Ngram only covers books) for ‘statistical modelling‘. ‘Mathematical modelling’ for some unclear reason gives a rather different result (sharp peak in 1980s and then falls back, but still much higher than previous levels), but the point is much the same: ‘modelling’ is a relatively recent concept that only really took off at the end of the last century. Before that, fuddy duddy scientists did what they had always done, science.
Although admittedly my approach is rather purist, I would argue that it is impossible for anyone to give informed consent to receiving one of the Covid-19 “vaccines”. That is because no one in the entire world – including, explicitly, the vaccine manufacturers – knows how they work, what they do, or what their short-term, medium-term and long-term effects might be. Absolutely no one is “informed”.
To my mind the only certain effect of those concoctions is to enrich a whole string of people, from the employees and shareholders of Big Pharma, through doctors, nurses, casual labourers hired to administer the “jabs” (like it’s hard), and everyone in government and the NHS who gains from the huge sums of taxpayer money (and borrowing) so gaily paid out by Mr Johnson and his accomplices.
The following cartoon expresses my feelings very clearly (don’t look at it if you are offended by bad language):
https://a.disquscdn.com/get?url=https%3A%2F%2Fpopularresistance-uploads.s3.amazonaws.com%2Fuploads%2F2020%2F05%2Fhippocraticoaf-768×733.jpg&key=nlp4Oo-TeQXn6aR_PAa70w&w=600&h=479
Tom, I tried your no-one in the world with capacity to give informed consent – least of all children, least of all the jab makers since no long/medium/short term safety trials have been conducted – on my MP, this when the child jabbing was first mooted.
Water off a duck’s back. Both cartoons spot on.
Contrary to official propaganda, your MP does not represent you in any way. MPs are employees of private corporation – the political parties. Until such parties are made illegal, we cannot have democracy again.
As Ben Greene wrote back in the 1960s or 1970s,
“Today the country is governed entirely by private organisations under no legal or public control. These organisations are the political parties…
It was in the General Election of 1874 that the modern party under caucus control became a decisive influence in our parliamentary constitution. In 1906 it achieved complete power. From 1906 onwards, constitutional law meant nothing, and everything was decided by a secret, irresponsible party committee which we know as the Cabinet…
“The position today is that the parties, by destroying the freedom of election, now control the House of Commons. By this control the only Ministers who can gain the confidence of the House of Commons are the party leaders themselves. By their control of the House of Commons, they can never be impeached…
“The only way to restore constitutional government is to restore the freedom of the M.P. This means that the political monopoly established by the parties in nominating candidates must be destroyed. It means further that the whole concept of party government must be destroyed, and that constitutional government in Britain must be based on national principles…
“If you vote for a party government, you are voting for unconstitutional government”.
“If you vote for a party government, you are voting for unconstitutional government”. Absolutely. There’s is no party I could support now.
Is Dr No right in supposing that the modelling you did was limited to fitting equations to the data, and did not extend to making extended (and so extrapolated, and very possibly wild) predictions based on those equations?
My models weren’t data fitting: they consisted of sets of simultaneous partial and ordinary differential equations that expressed (I intended) physio-chemical truths: conservation and rate statements mainly. But they needed parameter values. When my supervisor and I agreed that some values from the literature weren’t good enough for me to use confidently then it was off to the lab.
Then I could make predictions, the intention being that making predictions with my models was much quicker, cheaper, and safer than performing trials on big industrial kit. So this is like Tom’s point: “When an aircraft, a missile or a space vehicle is sent up, we trust science when it assures us that they will go more or less where intended.”
You might thus understand why I scoff at rubbish like Ferguson’s stuff being called “mathematical modelling”.
‘You might thus understand why I scoff at rubbish like Ferguson’s stuff being called “mathematical modelling”’.
I do indeed understand! Although strictly speaking it is mathematical modelling – just very badly done. And actually not worth undertaking at all, as the problem domain does not lend itself to accurate modelling because so very much is not known.
Ferguson, like “experts” and politicians worldwide, seems to have assumed that he could not go wrong (career-wise) by exaggerating the danger. Unfortunately, he seems to have been right about that.
not worth undertaking at all, as the problem domain does not lend itself to accurate modelling because so very much is not know
Zaktly.
When is a hospitalisation not a hospitalisation?
https://www.theatlantic.com/health/archive/2021/09/covid-hospitalization-numbers-can-be-misleading/620062/
When is a “case” not a case? When it is based on a positive result from a test that tells you nothing.
When is a hospitalisation for Covid not a hospitalisation for Covid? When it is based on a positive result from a test that tells you nothing.
When is a death from Covid not a death from Covid? When it is based on a positive result from a test that tells you nothing.
There seems to be a common factor there.
https://cormandrostenreview.com/report/
Thank you, Dr No, and all, for this little corner of sanity on the internet. I don’t get here as often as I would like, but have enjoyed catching up with this discussion.
I have long suspected that our preparation for the anticipated arrival of a new ‘flu’ from China (they always come from China, don’t they?) would have been much better led by historians than by scientists. At least they might have cautiously placed matters in context, recognising the increasing uncertainty as we look, for example, back to epidemics which occurred before the identification of the influenza virus.
The kind of epidemiology Dr No describes looks a very humble science. The science of practical doctors like William Budd, William Pickles and Edgar Hope-Simpson seems to me a kind of ‘live history’. These men may all have studied past epidemics, but they also had the foresight to track epidemics as they unfolded, seeking to understand, to test their own understanding, and to provide material that might help later generations understand. My impression is of men who recognised that perhaps only one or two pieces of the puzzle were within their reach, but if they could just locate those, then our knowledge would be advanced.
My first encounter with modern ‘epidemiology’ was during, or immediately after, the Iraq war. Fiercely opposed to the madness I had seen develop over the preceding year, furious at the lies and resulting deaths, I was much impressed by the work of ‘doctors’ from Johns Hopkins University who used ‘epidemiological methods’ to estimate the death toll. Of course, being young and indignant and on the same side as the researchers, I failed to notice the implausibility of their estimates. They were using epidemiological methods – they had to be right!
Iraq was not an epidemic. But the injustice of what was done there is not best highlighted by wishful thinking and dodgy statistics.
When did epidemiology become so corrupted? Was it ‘public health’? Is epidemiology now the study of diet? I get the impression that some of the Covid ‘epidemiologists’ appear to have a background in dietary ‘science’. But eating chocolate is no more an epidemic than is dropping bombs in the desert.
Great conversation, thank you all!
Tom, I love the cartoons!
Just wanting to add ; all this for something with a 99.6/7/8% survival rate, and, for many, from a malady apparently easily mistaken for hay fever….
Cui bono…and whatever the Latin is for ‘who’s benefiting from the benefiters’ benefiting’… Note bene their truly ghastly intentions. The global survival rate from the Gloop Deployment (excellent humour in a dark situation, Dr No) is way below 99.8%. God help our children…
Thank you all for your comments.
It is true on one level that it is an oxymoron to give informed consent for something on which there is no information (specifically, on medium to long term effectiveness and side effects). But it is also true that, in a pragmatic sense, we can be informed that we don’t know about medium and long term risks and benefits, in the same way that an investor can be informed that the value of his stock may go down as well as up (Dr No uses the investment analogy deliberately). Given knowledge of the uncertainty, the individual giving or withholding consent is in effect taking a gamble, hoping that whatever course of action he or she chooses will produce maximum benefit (health, profit) and minimum harm (illness, loss). And that’s why it needs to be the individual’s decision: no one has the right to gamble on another’s behalf. On the other hand, the individual does have the right to gamble with is own money, or health, and woe betide any health fascist or coercive healthist who tries to take that right away.
None of that is to deny for a moment the importance of the financial gain some will make from plugging the vaccines. For many of them, it is the perfect gamble, all gain, and no pain (as in no liability). To use that hideous phrase, what’s not to like?
dearieme – perhaps your mathematical modelling fits Misa’s excellent concept of humble science: the honest endeavour of nibbling away at what we don’t know about the natural world to get a better understanding. If something doesn’t seem right, you nibble away at that bit. This could not be more different to – as SAGE have just done – making sweeping statements like hospital admissions ‘could be’ as high as 7,000 per day by next month, a cue for Mishal Husain to wring yet more grey tears from her diabolical dishcloth of covid despair.
A useful link to the Atlantic article, well worth a read. The original paper is here (a pre-print, and surprisingly difficult to locate – Dr No was on the point of declaring the Atlantic article to be bogus), and while it is true the study population is VA (Veterans Affairs), and so American (different ways of doing healthcare) and mostly old and male, and the definition of severe disease is open to debate, the findings are nonetheless consistent with the emerging evidence suggesting substantial – and, some might even say, fraudulent – official over-counting of covid cases.
The covid PCR test can of worms has been doing its own internal polymerase chain reaction, and now has so many worms in it that it is about to explode. The consequent mess will form the basis of a new post.
Dr No, I was perfectly certain that counts of “cases” admitted to US hospitals – and dying there – were grossly exaggerated as soon as I read, about a year ago, that the federal government was handing out up to $100,000 per case. I know enough about hospital administrators and their perpetual want of funds to see that this could only lead to drastic over-counting. As Tom Naughton (among other) says, “Follow the money!”
“State-by-state breakdown of federal aid per COVID-19 case”
https://www.beckershospitalreview.com/finance/state-by-state-breakdown-of-federal-aid-per-covid-19-case.html
“State of Alaska receives $1.25B in federal COVID-19 relief”
https://www.ktuu.com/content/news/State-of-Alaska-receives-125-billion-in-federal-COVID-19-relief–569877881.html
“If something doesn’t seem right, you nibble away at that bit”.
Very sensible, Dr No! Mony a mickle maks a muckle, if you’ forgive my provincial dialect. You remind me of Isaac Asimov’s classic remark:
“The most exciting phrase to hear in science, the one that heralds new discoveries, is not ‘Eureka!’, but ‘That’s funny …'”
I’m sure Dr No will be able to provide the correct figure for Jan-June 2021’s (deemed) covid deaths, but considering the non-use of the same measuring method for vax deaths vs covid deaths – i.e. dying within 28 days of a positive test – I find it more than alarming (and appalling) that, using the similar yardstick, 30,305 people have died within 21 days of their vax (ONS) between Jan and June 2021, ‘but that’s obvs ok and not to be mentioned’. Plus, putting that info, even as a screenshot of the ONS’s own page, on social media results in it being censored and an instant ban. Must be true then…. And we have a major problem…
Annie – while you were commenting here, Dr No was putting together his latest post (Cavernous Numbers Meaningless to Man) which looks at the (un)reliability of any numbers that rely on PCR tests to make them covid numbers. The up to 28 days interval is one of the problems, though not the main thrust of the post, which is about Ct values. The bottom line is that we don’t know what the numbers are, only that they are grossly exaggerated, possibly, as no doubt Tom will agree, to the point of being meaningless.
The social media censorship is a great and growing evil which Dr No abhors. He avoids the problem by having his own blog, but that is not an option everyone wants to take up, so we are left with rampant unaccountable censorship. At least you can mention it has happened here, and if you can have the screengrab online somewhere, then you can add a link here (as Tom did for his excellent cartoons) using the link button above.
If only the Russians had had a good mathematical model of the Chernobyl reactor they might not have attempted their bonkers plant trial.
On the other hand, with a decent mathematical model they would never have built that design of reactor at all. A rough calculation on the back of an envelope would have been an adequate model to rule out that design.
And another thing. I played a role, though a minor one, in HMG’s analysis of Chernobyl. I was most impressed at the amount of information that arrived on my desk, and the speed at which it arrived. So as recently as 1986 part of our State apparat was capable of competence at dealing with a scientific/technological problem (indeed, one involving the secrets of another state).
What has happened since – why has it floundered so badly with Covid? You might say that a comparison of Thatcher and Blair casts some light – but are they perhaps just symbols of some more fundamental problem?
A bit late to this discussion, but anyway…
Science studies the real world, but to make sense of it requires theory, a simplification and abstraction — you might even say a model. The value of a theory depends on it making useful (true) predictions. With a good track record of successful prediction a theory can provide useful predictions for engineering design say. But a useful theory can, in a sense, look into the future, it can be extended to hypotheses: predictions that will test the valid scope of the theory. Some hypotheses will crash and burn, we have tested the limit. Other hypotheses are away with the fairies, so ungrounded in common sense that testing would seem superfluous. There is a middle ground where hypotheses provide testable predictions and ways of seeing the world that gain ground beyond our current perceptions. The important point is that predictions must be testable.
djc – never too late, one of the many reasons for having a blog is that it stays around. Comments can be added later, cross references to previous posts can be made, and it generally stands the tests of time. Unlike ‘the other place’, where the bird brains screech all day, each one louder than the last, until it becomes all noise and no signal.
Yes, predictions are at the heart of the scientific method. Einstein’s e = mc2 is a prediction. When we do an RCT, we predict there is no difference between the treatment group and the control group, and then test that null hypothesis. So how do we distinguish between these valid uses of prediction, and whatiffery? The whatiffery that predicts x million people will die of covid if this happens, or alcohol consumption will halve if the minimum unit price is set a x pence per unit? Perhaps the answer is in the word whatiffery itself: the moment the word ‘if’ appears (what if we don’t lockdown, what if we increase the MUP to 50p/unit), then we have moved into the realm of numerological fantasy, where the numerologist twiddles the dials to get results that he (and it usually is a he) finds to his liking.
The other distinction that springs to mind concerns the open vs closed nature of the prediction. When we use prediction to do an experiment, or fire a rocket at the moon, the prediction is closed, to the extent it has an endpoint: the experiment comes to an end, the rocket either does or doesn’t land on the moon. Whatiffery is more open ended, but not completely so, as in time we compare the actual outcome with the predicted outcome, so open vs closed isn’t at the core of the difference, but perhaps has something to do with it.
Why does all this matter, we might well ask? It matters to the extent that we can spot whatiffery, and warn against its unreliability before it is too late. Imagine a world in which we could demonstrate that Fergie’s predictions (and many of the subsequent ‘predictions’ were unreliable whatiffery right at the moment they appeared? We might have had a very different pandemic. And yes, that last but one sentence is in its own way an example of whatiffery (what if we had been able to spot whatiffery…), but Dr No excuses it on the grounds it is retrospective whatiffery rather than prospective whatiffery.