
Just Another Seasonal Flu Like Illness

For some time, Dr No has been moving, or perhaps driven, to a determination — he uses the word with at least two of its meanings — that the only sensible considered response to covid–19 is to treat it as just another seasonal flu like illness. He knows full well that some will be of like mind, but that many — they know who they are — will react violently, in some cases with extreme violence, to any such suggestion. Dr No is a heretic! Burning at the stake is too lenient a punishment for heresy! Let him be hung, drawn and quartered, and his eviscerated staked body be displayed as a grim reminder to those who contemplate such heinous heresy! So it behoves Dr No to explain how he came to this determination.
The first question is whether covid–19 a seasonal flu like illness, and the answer is yes. On the basis of what we have seen so far, it is clearly seasonal, though that is subject to a projected — indeed expected — bump in cases over the next few months. It is a respiratory virus, like flu, it is contagious, like flu, and its severity affects people differently, like flu. The details vary — it is a different virus, its transmission has minor differences, and the differential severity varies, but, by and large, it is not at all unreasonable to say it is a seasonal respiratory virus not unlike influenza. There is no particular defining feature that makes it stand out as in some way being notably different.
The second question is whether covid–19 can justifiably be called just another flu like illness, in the sense that it is nothing exceptional. Dr No can already see the airborne bricks heading towards his window. But let us try an look at this sensibly. To do so, we are going to use the practical epidemiologist’s favourite number, all cause mortality. Those familiar with medical research will recall that this number is the most robust number of all, and is to be preferred when comparing say treatments effects, because it solves the significant problem of misattribution and misclassification (deaths being counted in the wrong place). We can use all cause mortality in the same way, to look at covid—19’s effect on mortality. Note this is nothing fancy. These are just basic counts of deaths, with no fancy adjustments, no conversion to rates, no attempt to determine excess deaths, no numerology, just the bare counts.
Using ONS weekly deaths available in a set of spreadsheets here, Dr No has summed the annual total deaths for the last ten years, with the year running from August to July. There are two reasons for choosing this as the year. The first and obvious one is that we are at the end of August now, and so have reasonable provisional death counts for up to the end of July for 2020. The second one is because this Aug-July year is the year ONS use for their excess winter mortality calculations. While we can’t immediately do a like for like assessment of excess covid–19 mortality, because ONS defines winter for these calculations as the period December to March, and the excess covid–19 deaths happened later in the year, it is likely we will in the future be able to do such a calculation, by re-defining the winter period to include the covid–19 season, and it seemed sensible to Dr No to set up the data that will allow it to be readily used for such a calculation.
What do we find? Figure 1 is the total number of deaths for England and Wales for the last decade (the maximum duration of data available on the ONS webpage), for the August to July years. The first thing we notice is a slight upward trend, and this is confirmed by adding a trend line as shown. This slight upwards trend over the last decade has been widely noted and confirmed (actual numbers are slightly different, but not significantly, to Dr No’s ONS based counts), and is likely due to a combination of population growth (more people) and a demographic shift (more older people).
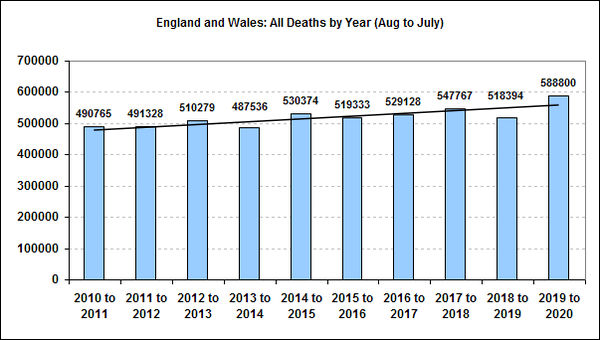
Figure 1: Annual (August to July) death counts for England and Wales for the period 2010-11 to date, with trend line added. Sources detailed and linked to in text.
The second thing we notice is a visible year on year fluctuation. In particular, 2018-19 was below trend, and 2019-20 (the year of covid–19) is above trend, though not strikingly so. In general, see-sawing above and below the trend is to be expected: if more old folk die one year, there are less to die the next; if more survive the year, then there are more to die the next, so some of 2019-20’s deaths will be ‘carried over’ deaths from 2018-2019. Nonetheless, 2019-20 is the year with the largest number of deaths in recent years. The key question is whether the increase is exceptional, or instead it is just another year.
We can get a good enough answer to this crucial question by using the trend line to estimate (yes, Dr No is using low grade numerology here, but it is very transparent, and you can make up your own mind as to how valid it is) how many deaths we would expect in 2019-20, based on recent trends, and compare that to the actual number of deaths. What we find is the trend predicts around 559,000 deaths, and in fact there were 588,800 deaths, an excess of around 29,800 deaths.
This number, around 30,000 excess deaths, is not inconsistent with a downgraded (for over-enthusiastic over-egging) official covid–19 death count, but with one key difference. Recall that we deliberately used all cause mortality, to avoid misattribution and misclassification biases (calling a non-covid–19 deaths a covid–19 death when it isn’t), and so that 30,000 or so figure will also include all the excess non-covid–19 deaths caused by lockdown, not seeking medical help, and delayed treatments. Nonetheless, we have traded what folk these days call granularity for simplicity and robustness, which means we do not know how many of the 30,000 were true covid–19 deaths, and how many were potentially avoidable lockdown deaths — you guess is as good as Dr No’s at this stage (in due course we will get a better idea, once mortality by cause data become available), but he suggests, as a starting point, maybe as many as half of the excess deaths were not due to covid–19, but were instead caused directly or indirectly by lockdown.
Is between 15,000 and 30,000 true excess covid–19 deaths exceptional? Dr no suggests not, in the wider scheme of things. Any untimely death is a tragedy, and Dr No’s heart goes out to those who have lost loved ones, but we have to be sensible, and accept that some of those excess deaths were so called dry tinder deaths (the slightest spark — tiny clinical insult — sets the tinder on fire — patient dies), a possibility made more likely by the lower number of deaths in 2018-19. Furthermore, 15,000 to 30,000 deaths is not a huge proportion of all deaths (2.5-5%), and such year on year fluctuations happen, especially in bad flu years. In recent years, excess winter deaths associated — albeit by numerological methods, because flu deaths, like covid–19, are not reliably recorded in death certificates — to flu have ranged rather wildly to say the least, even when using the same methodology (see here, here and here, but that’s PHE for you, and note these are England only estimates, not England and Wales), with the number ranging from 7,371 to a 34,300 depending on both season being estimated, and the year the estimate was made. Cobbling together some crude averages from these sources — it’s the best we can do with what we’ve got — we get counts ranging between 11,201 and 31,315 (2014/15: 31,315; 2015/16: 11,201;
2016/17: 16,883; 2017/18: 24,248). These figures are nonetheless broadly in line with another earlier estimate, of between 7,000 and 25,000 annual flu deaths between 1999 and 2009. Figure 2 shows the PHE numbers visually, along with a mid-estimate for covid–19 deaths based on Dr No’s analysis presented here. Dr No’s covid–19 estimate is in the middle, with flu seasons having lower flu deaths, and two seasons having more flu deaths.
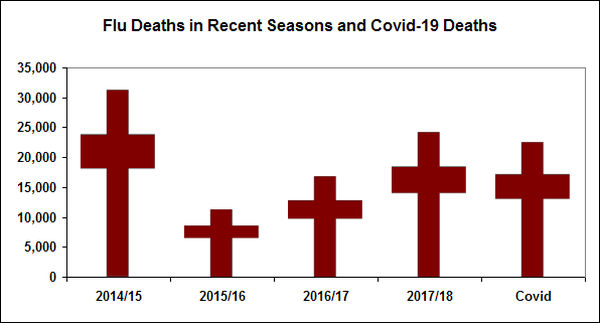
Figure 2: Recent seasonal flu deaths (England only) and estimated (22,500, half way between 15,000 and 30,000) covid–19 deaths (England and Wales) to end July 2020. Source of flu numbers linked to in text.
So is covid–19 really just another seasonal flu like illness? On the basis of the numbers — deliberately simple, deliberately robust (with the exception of the PHE flu death estimates, which are decidedly flakey, but are the best we have for recent years), deliberately transparent, no fumbling around with confused shambolic undenominated test results, no trying to guess the real cause of death, just all cause mortality one a year, because sometimes less is more — presented here, it seems hard if not impossible to argue that covid–19 is exceptional. It seems entirely reasonable to call it just another seasonal flu like illness. That is not of course to say for a moment that for every patient covid–19 is trivial, but instead to put it in its rightful place in the wider picture. For some patients, either flu or covid–19 can be anything but trivial, and both can be fatal. But — the key point — covid–19 is not wildly exceptional. Its mortality is, by and large, and give or take, of the same order of magnitude as flu, low to middling tens of thousands per season.
In which case, why on earth did we lockdown? The answer is panic — Fergie farted, the cabinet panicked. On a charitable view, one might see, if not necessarily agree with, the reason for the government’s early panic in March. But we have now moved on, a long way on, and have a far better understanding of what actually happened, in contrast to a numerological guess at what might happen. Now is the time, Dr No suggests, to get back to normal, and treat covid–19 as just another seasonal flu like illness, managed just as we manage any other seasonal flu like illness. We can — and should — do for covid–19 as we do for flu, up to and including deploy a vaccine if and when one becomes available. Indeed, we should do nothing less, and just as importantly, nothing more.
But…..in normal flu seasons we don’t close schools, pubs, shops etc. and make other huge changes to our behaviour.
Is there any way of estimating (roughly) what the excess death figures would have been, had we carried on as in a normal flu season ?
And do normal flu seasons lead to situations as severe as that seen in Bergamo ? I think panic in such circumstances is fairly understandable……
A manufactured ‘panicdemic’ which no doubt has wreaked havoc and harm, is now slowly coming to light as such — as people grow tired of the media hype, government flip flopping and daily life encroachment —which will become increasingly more apparent as we head into winter, with for many, its grim economic outlook.
Tony – the best we have here is the international comparisons, and as has been said here and elsewhere, these ‘natural experiments’ are not without their problems – but the are the best we have (good answers to the right question rather than exact answers to the wrong question again). Comparing and contrasting Sweden with other Nordic countries, the UK nations and Mediterranean countries is at the very least interesting. Northern Italy may also be a special case, for several reasons: links with China, air pollution, demographics (old), Latin ebullience (normally so very welcome) and lifestyle.
The problem with estimates, even rough ones, is that they very quickly turn into what-if numerology, and so inherently become unreliable. The virtue of this post, if it has virtue, which of course Dr No thinks it has, otherwise he wouldn’t have published it, is that in that the first part, summarised in Figure 1, it uses simple robust and verifiable counts. If there was an epidemic, it should be visible in Figure 1. The second part of the post, summarised in Figure 2, is weaker, because the PHE estimates of excess flu deaths are numerology based (but are the best we have etc etc).
In due course it should be possible to do ‘proper’ excess death calculations, based on the ONS excess deaths methodology, but with a different time frame, as ONS use December to March as winter, and clearly the covid deaths happened mostly outside that period. Dr No is hoping he will have time to take this further soon, but don’t hold your breath!
James – whether the ‘pandemic’ was in fact nothing more or less than a panicdemic is exactly the key question raised by this post. Dr No suggests that it is more than even odds that pandemic or no pandemic, it was also beyond doubt a panicdemic (‘Fergie farted, the cabinet panicked’).
But even in Sweden, surely life did not continue in anything like the way it does in a normal flu season ?
Universities and high schools were closed, gatherings of more than 50 people were prohibited, and people changed their behaviour in ways that they don’t do (as far as I know) in a normal flu season. I saw a quote recently from Tegnell (which of course I can’t find now) in which he said that mobility had fallen in Sweden by roughly the same amount as in Norway.
On the “Latin ebullience”, based on my very limited experience of Northern Italy on skiing trips, I’m not sure this is a fair characterisation of Northern Italians. There may be more handshaking and kissing than is normal in the UK and more mixing within families, but life struck me as being quite formal and reserved in some ways. But, leaving aside the stereotyping, ebullience and all the other factors you mention such as pollution have been there during normal flu seasons, but the effects don’t seem to have been as catastrophic.
Given the absence of a real “control group” where life has carried on as normal, I think it’s very speculative to suggest that COVID is just another seasonal flu-like illness. How about “It’s flu, Jim, but not as we know it” ?
Tony – ebullience was rather too glib shorthand (but meant in a complementary way) for the Latin temperament and I agree Northern Italians are different to Southern Italians, at least based on my Italian travels. In fact, if I recollect, the Italians themselves have three Italys, North, Middle and South.
There has been some uncharacteristic hand-wringing (as opposed to the more normal firm but open humility) among the Swedes of late, but there was also an interesting article in the Spectator a few days ago by a Swedish doctor saying pretty much Sweden had covid done and dusted -‘Sweden ripped the metaphorical band-aid off quickly and got the epidemic over and done with in a short amount of time’ (the google cache version of the US edition is the way to get the article):
https://webcache.googleusercontent.com/search?q=cache:8YCxaLHcU18J:https://spectator.us/dangerous-covid-swedish-doctor-perspective/+&cd=3&hl=en&ct=clnk&gl=uk
The article is also particularly interesting in that it touches but doesn’t expand on the very interesting question of what percentage of people need to be immune given naturally acquired immunity (which will involve various selection effects) to gain herd immunity, compared to the percentage needed from a vaccination program (random vaccination, people vaccinated whether at risk or not, so you probably need to have a higher percentage). So far as Dr No is aware, this aspect of vaccine science has not been adequately studied.
Dr No is perfectly content with “It’s flu, Jim, but not as we know it”, as it doesn’t suggest or imply that it is exceptional, just that it is (like) flu, but a bit different, which is pretty much what the post says. The ‘just (another)’ – well, you know why Dr No added that…
A propos Tony Holmes’ very reasonable questions, it is surely hard to compare Covid-19 with flu if only because no saturation “testing” has ever been done for flu.
There is great uncertainty in all countries over the prevalence of flu and, especially, the number of deaths it causes. Estimates I have seen are all over the place.
Yet throughout 2020 governments and official institutions have been publishing exact “case” and “death” figures for Covid-19 from one day to the next – in spite of the fact that there seems to be no reliable test for the presence of the virus, let alone whether it has killed someone.
I wonder how many “cases” and “deaths” officially attributed to Covid-19 are actually due to flu or some other disease which is not so desperately sought after.
Tom – All good points which Dr No generally agrees with. Covid may well be what Dr No calls a Trumpdemic, ie you do more tests, you find more cases. If we did the same thing for flu, we might well find we had a flu Trumpdemic. You are absolutely right, estimates of flu deaths do vary widely, and I hope this came across in the post (‘excess winter deaths associated — albeit by numerological methods, because flu deaths, like covid–19, are not reliably recorded in death certificates — to flu have ranged rather wildly to say the least, even when using the same methodology’ -if you click on the links and go to the sources you will see wild variations even within different year versions of the same report, using the same methodology).
Yes, official figures have always seemed very precise, very day by day, but then again they admit to over and under-counting eg the sudden recent ‘redjustment’ to UK deaths to exclude some of the the once had covid actually run over by a bus deaths. The ‘desperately seeking covid’ effect is what Dr No called Hot Stiff Bias a while back. Frankly, we have little if any idea of real case numbers, let alone rates – haphazard sampling often with with selection bias+++, no denominator most of the time, a dodgy test (see posts passim) that may detect defunct historical virus RNA of no clinical relevance etc etc – and not much better an idea of deaths.
That is why Dr No used all death counts – it simplifies, but it also solves the misattribution/misclassification problem. The basic logic of this post at its simplest is: if there was a pandemic, there should be more deaths: is that what we observe? The answer is yes there is a small blip, but it is not exceptional and is for example much the same as seen in 2013-14 => 2014-15, when covid was not around. Ergo covid is not exceptional, it is instead just another seasonal flu like illness/flu, Jim, but not as we know it.
For many weeks now Belgium has seemed to be an outlier. Have you any idea why? Could it be an artefact of reporting cause of death?
Ignoring recent immigrants, the Belgians are more or less the same people as the Cloggies, the Krauts, the Frogs, and us. So it’s unlikely that any ethnic/racial burble will explain it, nor weather, geology, age distribution. What’s up, doc?
Dearime – Belgium is indeed an apparent outlier, at least in deaths per million people:
The reason is believed to be ‘desperately seeking covid’ ie Belgium has very inclusive – or perhaps we should say lax – criteria for including a death as a covid death, hence more deaths are attributed to covid. See this Brussels Times article for more details.
Dearime – Perhaps also worth adding (again) that this is why Dr No used all deaths in the post – solves the misattribution (over/under-attributing deaths to covid-19) problem. If Belgium were to do a year on year all deaths chart akin to Figure 1 in the post, they may well find nothing exceptional was going on.
Regarding Tony’s fair point its also worth noting that at the least Sweden disproves the numerology which the “worst case” scenarios we’re based on; the assumptions made by imperial were applied to Sweden by upsella uni and the model gave them 10x the deaths and ICU requirements that were actually recorded. It’s also worth noting that Malmö recorded lower deaths than Copenhagen despite being in the same conurbation and Copenhagen having a lockdown. Certainly food for thought.
But it’s impossible to prove a negative: what would have happened in the absence of an organised control.
It’s hard to dispoe
I think unless I am missing something we are all on the same hymn sheet, which if I can be as bold as to summarise is:
(a) covid is new, poorly understood but seems to be roughly of the same order of magnitude in adverse effects as a bad flu season, when we don’t do anything exceptional, yet covid did prompt truly exceptional behaviour, with uncertain benefits (that we can’t prove to a gold standard one way or the other), and many proven harms that have damaged health, education, society and the economy.
(b) while we don’t have and are most unlikely ever to have gold standard quality evidence, we do nonetheless have the natural experiments with Sweden and Italy among many throwing up interesting results, and it behoves us to make as much sense of these natural experiments as we can, with due regard for the potential biases and other unknowns.
All this is a perfect example of the application of Dr No’s favourite epidemiological maxim, better a good enough/approximate answer to the right question (like the one we are asking here), rather than an exact answer to the wrong question (physics lab tests on mask materials springs to mind, can’t imagine why).
Some useful charts/tweets from Helen McArdle on twitter, approaching the question, and presenting the results, in a slightly different way, based on Scottish data. Again, the conclusion appears to be that covid is like a bad flu year, rather than something exceptional.
https://twitter.com/HelenMcArdle3/status/1299692010606080006
When I’ve asked medics about the response (in particular CPR updates and risk assessments) I’ve found that the only answer given is that this is new. They seem unable to give anything more when I too suggest that this is in the same ballpark as flu like illnesses we have always had. Either they have been sleep walking for years or have simply accepted the narrative with little or no scrutiny.
Great post. Thanks
Rick – I’m afraid there is nothing to stop medics from being caught up in the collective madness. It could even be said that they – one thinks of the milk curdler, for example – along with certain academics, have been the high priests of the madness. Medicine is an art and a science and doctors who are temperamentally science-lite feel no particular obligation to engage in sceptical rigour. For some doctors, medicine is above all else a calling, and when you are called, you don’t faff about asking difficult questions, you do what you are called to do. And finally there is the not so small matter of self-interest, the need to manufacture illness to stay in work. This is a particular problem in psychiatry (because of the lack of basic medical science and diagnostic rigour, it is rather too easy to make up new illnesses) but the same process is at play in all branches of medicine. A good general example is statination (everyone’s cholesterol is too high so we’d better prescribe statins for everyone); another is PSA testing (all males over a certain age have probably got prostate cancer so let’s test them and treat those over a certain (arbitrary) level without asking too many questions about how much good/harm we are doing).
The saving grace is that because of its scientific roots, western medicine allows sceptics. While a majority may worship at the altar of convention (your sleepwalkers who simply accept the narrative), and some sceptics are treated as heretics, by and large, those who want to question are allowed to question. Were it not so, this blog would not exist.
The PCR tests are not very reliable, especially kits manufactured in certain countries (allegedly). I am amazed that test kits appeared all over the world almost instantly, as if by magic (or advanced preparation?), but also how these kits can distinguish between Covid19 and all other coronaviruses.
Flu vaccines are notoriously ineffective in over a third of cases, having to be altered every year to cope with mutations. Will a Covid19 vaccine be any different? Will a new vaccine be needed for Covid20, Covid21, etc.?
Ed – The PCR tests are indeed dodgy, see posts passim. The vaccine is at the moment the triumph of hope over experience, in that so far as I know, there has never been a successful coronavirus vaccine. That may be partly because we haven’t needed one (SARS and MERS were got under control by other means, and ‘ordinary’ colds haven’t yet produced a need for a vaccine) but it is also possible coronaviruses are hard to vaccinate against, and/or the vaccines are prone to complications. Of course if we do get a safe effective vaccine it will be a game changer, but I’m not holding my breath. Even if we do get one, it may well as you suggest have the same problems as flu vaccines.
I’m uncomfortable with the claim that CV-19 is similar to flu at this stage, as the comparison being made is the progression of a virus through a society which has massively modified its behaviours and one in the case of flu where we only make local modifications such as keeping children off school and staying away from work for a few days.
Anecdotally I saw my first face covering on UK public transport on Feb 14th. There’s some evidence that R went just below 1 around 16th Mar with homeworking already in place for many, ski holidays and cruises cancelled, large weddings, medium funerals, church services, indoor music and sport all cancelled or scaled back. Education curtailed, many voluntary social gatherings among the more educated had ended a week before LD.
So it’s really a flu vs a ‘brakes-on’ CV19 comparison.
I do note that deaths in the last 104 weeks are around 30k higher than the previous 104 weeks in the UK. In Sweden, it’s about the same. Well done Sweden.