
Hot Stiff Bias

The news event of the week so far, apart from all the other news events of the week so far, is yesterday’s release by ONS of weekly deaths for 2020. For total deaths, weeks 1 to 12 are unremarkable, week 13 showed a none too remarkable rumble in the jungle up-tick, and then it happened in week 14 — the numbers went through the roof. This isn’t an exponential rise, it’s a stratospheric rise, like a rocket taking off for space.
This sudden rise, up to 16,387 from 11,141 the week before, in the number of total deaths is the remarkable event — see the chart below — but for some unfathomable reason the mainstream media focused more on a similar but less dramatic rise in the number of covid–19 deaths, up to 3,475 from 539 the week before.
If we look closer at the figures, some curiosities appear. Firstly, we should remind ourselves that the hardest of the data here are those for total deaths. Stiff counting is pretty basic, with the only minor irregularities being occasional delays in registrations, and even these will in time sort themselves out. Stiff counting by cause of death, on the other hand, is more prone to bias, since it relies on the doctor’s interpretation of the cause of death.
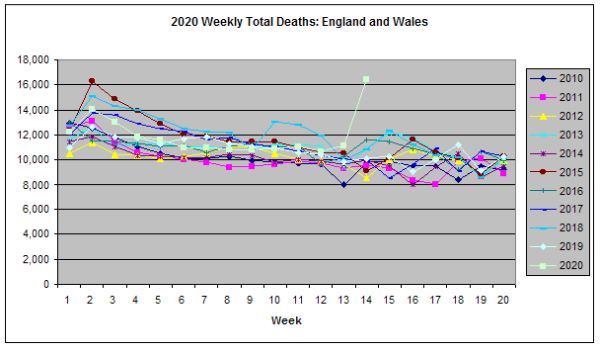
Figure 1: Weekly total deaths 2010–2020. Source: extracted from ONS data sets here.
One of medicine’s more hidden features is that despite all the hue and cry over evidence based medicine, it is still a practice of fashions. Indeed, evidence based medicine is a current fashion, albeit a sensible and long overdue one, like warmer underwear in the colder months. Treatments come into vogue, and then fade away, like grommets for middle ear disease in children, or don’t, like statins for the primary prevention of cardiovascular disease. But it is not just treatments that are subjects to the winds of fashion. Diagnoses are also prone to get blown into and out of favour. Psychiatry, with it’s lack of lab based diagnostic tests, is the most affected specialty, but others are by no means immune.
The effect is that when a diagnosis becomes ‘hot’, and so more talked about, it’s incidence increases, simply because it is on everyone’s mind. This is known as hot stuff bias – rates go up when the diagnosis is fashionable and topical. When the matter at hand is the diagnosis of the cause of death, we might call this bias hot stiff bias. If the death has any features suggestive of the ‘hot’ condition, then it becomes a ‘hot stiff’ and is more likely to have the hot condition included on the death certificate.
The ONS covid–19 death numbers are counts of all deaths registered with covid–19 anywhere on the death certificate, so we don’t know whether these are deaths from, or deaths with. Nor do the death certificates necessarily indicate (and nor is any separate count made of) whether the diagnosis was confirmed by laboratory testing (and that might still be a death with not from) or just a clinical diagnosis, based on the history and possibly — in the current crisis, this requirement has been removed — examination of the deceased. In both cases, but especially in the latter, there is more than enough reason to suppose the current ‘hotness’ of covid–19 is more than enough to explain at least in part the sudden rise in the number of covid–19 deaths.
Unfortunately, there is at present no way to determine the extent to which hot stiff bias is currently inflating the numbers of covid–19 deaths. Because of this, we might even say that the rise in covid–19 deaths is something of a red herring that we can leave to the mainstream media, in which to get its talons caught up, until such time that we have better reporting of the causes of death. So let us return instead to the much more robust number, the total numbers of deaths.
What we find is that, even if there was very little hot stiff bias at work, and most of the alleged coivid–19 deaths are true ‘deaths from’ deaths, there are nowhere near enough extra covid–19 deaths to explain the extra numbers of total deaths. Between weeks 13 and 14, covid–19 deaths went up by 2,936, while the total deaths went up by 5,246. That leaves at least 2,310 extra deaths not accounted for by the rise in covid–19 deaths.
One possibility, somewhat ironically, is that covid–19 deaths are being under-reported, and this may yet turn out to be the case, though given the ‘hotness’ of covid–19, and the fact it gets counted even when incidental so long as it mentioned on the death certificate make this unlikely. Instead, we have to consider what other factors might be at work that increase overall mortality. We should note here that this excess of at least 2,310 extra deaths is considerably more than the normal week on week variation, which is typically — see Figure 1 — around 1,000, though it does vary, and at times is closer to 2,000.
The most likely explanation, Dr No suggests, as at this stage no more than a working hypothesis, is that covid–19 is indirectly causing these deaths. These are the deaths caused in part by the displacement and dislocation of normal health care caused in the massive shift to covid–19 care, and in part by the disruptive effects of the lockdown on the normal social machinery and networks of daily life. They are the collateral damage, the collateral deaths.
The other possibility we cannot rule out is that these unexplained excess deaths will turn out themselves to have been a red herring, a sudden and soon reversed spike in excess deaths, part of the normal, albeit rather exaggerated on this occasion, week on week variation. Indirect covid–19 deaths and random effects are not mutually exclusive, such that both might be in play.
Recognising and explaining the early stages of epidemics is one of the hardest tasks in ‘live’ or ‘real time’ epidemiology, so much so that it all too often impossible to form sure and certain conclusions on the basis of early up-ticks, even when they are very striking. There is a real and significant risk of reckless over-reaction, from blind panic and a universal cry that ‘something must be done’. Much better, Dr No suggests, though not easy, is too sit tight and wait and see. And that, for now, is what Dr No is going to do.