
Covid Is Not the Problem
With the barrage of political and mainstream media talk of rising covid cases, new scariants and the urgency of vaccinating all, and then some — soon there will be talk of syringe drivers, pumping in covid vaccine in 24/7 — and not to mention Tuesday’s nodding through, not so much on a song and a prayer as on a laugh and a wink, by the blind horses in Westminter, of another six month extension of the Coronavirus Act, there can be little doubt that government is limbering up to implement Plan B. No doubt there is already a Plan C in draft, and so on, to pile Pelion on Ossa, forever and ever, world without end. But how are we really faring with covid these days?
Positive PCR tests are on the up, but then so too are the leaves in the sky, because it is autumn. Just because you find an oak leaf in your gutter, it doesn’t mean you have a forest of dying oaks at the bottom of your garden. The NHS — now entering its autumnal forecasts of doom phase — isn’t overrun with covid patients, which have remained pretty constant over the last two months. There’s even been a decline in covid admissions over the last few weeks, even if there is a more recent uptick — just as we expect in autumn. Alleged covid deaths — the ones that had a 28 day old oak leaf stapled to their chest — have also declined over the last few weeks, perhaps a less marked a decline than admissions, but still a decline. The current bout of covysteria is based solely on a swirling cloud of autumn leaves, and the MSM have become Hitchcock’s birds, swooping in the sky as they chase the swirling autumn leaves.
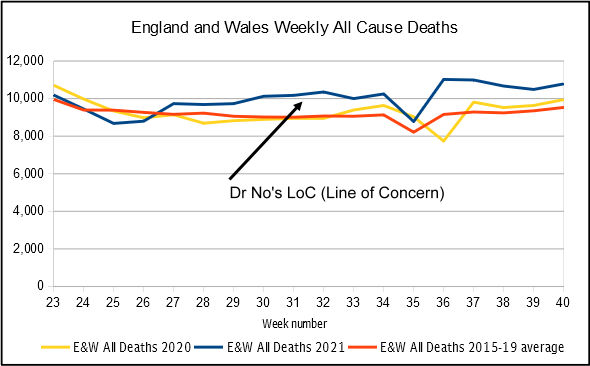
Where things are a little less encouraging can be seen in the chart at the top of this post, which shows weekly all cause mortality for England and Wales starting the week after ONS stopped reporting deaths by vaccination status. The three lines are 2021, and the corresponding weeks in 2020, and an average for the same weeks over the preceding five years, as a crude benchmark. 2020 — the first year of covid — was unremarkable. The weekly numbers of deaths hovered above and below the five year average. In contrast, 2021 shows a clear excess, starting in week 27, and persisting, and perhaps even increasing by a small amount, for every week except the bank holiday week. If we visually average the bank holiday trough and the following peak, the trend is clear. The data comes from ONS’s weekly figures, and while there might be minor revisions, these charts are pretty much based on what will go down in posterity. Nor are the numbers of excess deaths trivial, at an average of over 1,000 excess deaths per week since week 27, when the rise started. 1,000 a week is 4,000 a month, and so on. If the trend continues, the numbers soon add up.
What is causing these excess deaths? The short answer is we don’t know yet, as we will have to wait for more detailed cause of death statistics. What we do know, however, is that covid is not the sole culprit. In fact, it almost certainly isn’t even the main culprit. Figure 1 is an update of a previous chart, with deaths broken down into (a) non-excess expected deaths, being those non-covid deaths up to the five year average, or all non-covid deaths in the rare weeks when all deaths did not reach the five year average, (b) covid deaths and (c) non-covid excess deaths. This approach, and it is the only one possible given limitations in the data, makes two unlikely assumptions: firstly, that all deaths ‘involving covid’ were ‘from covid’, and secondly, that all covid deaths were necessarily excess deaths. Both of these assumptions will exaggerate the apparent impact of covid, making covid appear more of a problem than it is, which in turn will decrease the apparent number of non-covid deaths, making them appear less of a problem than, in reality, they are.
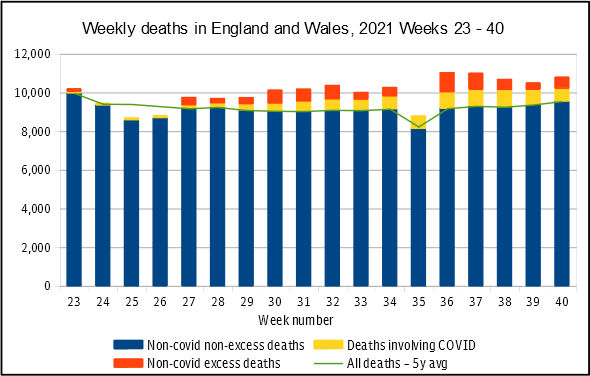
Figure 1: weekly deaths in England and Wales for weeks 23-40. Source: data downloads from this ONS page
In the first case — assuming all deaths ‘involving covid’ are deaths ‘from covid’ — means the yellow bar contains deaths that in truth were not ‘from covid’ deaths, the 28 day old oak leaf deaths. The yellow band should be smaller, and the non-covid excess deaths red band larger, by the extent that covid was over-represented as the cause of death. Dr No’s guesstimate of the extent of this misattribution of cause of death? Let’s say 50 %, or half of the alleged covid deaths were not in fact covid deaths. In the second case — assuming that all covid deaths were necessarily excess death — ignores the fact that some of these deaths were expected deaths, in that they were going to die anyway, and just happened to die from covid, rather than one of the other well known likely terminal illnesses. To correct this assumption, that all covid deaths are excess death, we need to move the yellow band downwards, so that some of the covid deaths show as expected deaths, and the consequence is the red, non-covid excess band gets larger. How much of the yellow band should be moved into the expected deaths zone? Nobody knows, so let’s hazard a guess: 50%, of half of the apparent covid excess deaths were in fact expected deaths. Figure 2 is Figure 1 plotted with these adjustments applied. It is clear that, with these adjustments, non-covid deaths, rather than covid deaths, are the predominate problem.
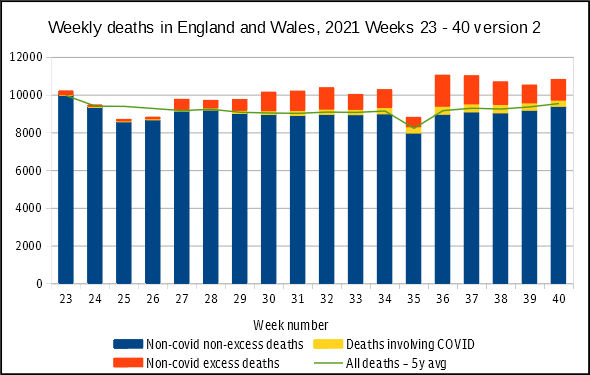
Figure 2: weekly deaths in England and Wales for weeks 23-40, with presumptive corrections applied. Source: data downloads from this ONS page, plus some data diddling by Dr No
Let us be clear, the 50% adjustments are no more than guesses. There are estimates of the extent of over attribution of covid as the cause of death, but they vary hugely, and frankly, none are yet conclusive. The how many alleged covid deaths were not excess, but expected, deaths question is even trickier, because it requires knowledge of when someone would have died regardless of when they actually died, in effect, another instance of Dr No’s infamous Schrödinger’s dilemma applied to prognosis: we cannot know the length of a piece of string until it is cut. But we can make estimates, as long as we make it clear that is what we are doing, because, as Dr No is wont to say, better an approximate answer to the right question, than an exact answer to the wrong question. With that in mind, Figure 2 tells us that, over recent months, it is non-covid excess deaths that should trouble us. Covid has become a distraction, a red herring, a wild goose chase, because covid is not the problem.
Brilliant! And thank you, Dr No; ‘ — the ones that had a 28 day old oak leaf stapled to their chest —’ had me crying with much needed laughter for a good ten minutes!!
No, covid isn’t the problem, but it’s been, and is, a mighty handy problem-procreator to hide plentiful plots, plans, and propaganda.
Here we go again; I listened just now, with BS-deflector turned up high, to the basic radio 3 news just now, offering ‘what’s happening, what might happen, and what definitely won’t happen in response to it’, meaning folks’ fear is piqued, solutions are hoped for, and when the it-will-never-happen-lockdown happens, it will be because the people pleaded for it and comply without question. One word on my lips; begins with b, ends in s, and has an s, t, d in the middle. And, quite…)
btw, for any of Dr No’s wonderful tribe who have Prime (I know, but) and haven’t seen the 2012 movie ‘Compliance’, I suggest a watch; pertinent for our times.
Indeed Dr No, I share your concern and am about to submit the following FOI request to the UKHSA which should help either eliminate or implicate one obvious potential cause for those excess deaths.
I am making the following request because while it seems from the latest weekly Covid -19 vaccine surveillance report that Covid 19 vaccines are effective at reducing hospitalisations and death due to Covid, we are still currently experiencing an abnormal amount of excess deaths for this time of year, which cannot be attributed to Covid alone.
As I believe it is extremely important that we eliminate the possibility that the vaccination program itself could be contributing to those excess deaths, ie causing more deaths than they save I would appreciate it if you could provide the following information to enable the “all cause” death rate to be calculated for the vaccinated versus the unvaccinated population.
Could you kindly provide the following information from the date of the commencement of the Covid 19 vaccination program:-
1) Weekly “all cause” death totals by date of occurrence, broken down in the age bands as per the Covid 19 vaccine surveillance report.
2) The associated vaccination status totals, based on the actual date of vaccination, again as designated in the Covid 19 vaccine surveillance report.
3) The total number of the population vaccinated or unvaccinated for each week, again broken down in the age bands as per the Covid 19 vaccine surveillance report.
I am no statistician, but I believe an answer to the above would help provide a clearer idea of whether these vaccines are contributing to this current excess mortality.
I would appreciate any feedback or further thoughts you may have on this matter, particularly if I have missed anything in my request
Four possible causes of non-covid excess deaths:
(i) The vaccines somehow add to the death toll (though not necessarily to deaths among the vaccinated).
(ii) The effects of NHS shutdowns are catching up with us because of diagnoses not made, treatments not given.
(iii) The fear and anxiety stimulated by government and the media, and the loneliness caused by the lockdowns, are taking a toll.
(iv) Reduced incomes caused by the lockdowns and by spontaneous reaction to the pandemic are causing deaths.
The following article by Dr Theodore Dalrymple has a good deal to say that is relevant to this thread:
“The World Always Surprises Us”
https://lawliberty.org/the-world-always-surprises-us/
Unfortunately, Dr Dalrymple takes a quite unnecessary swipe at Mr Putin, and ends his piece by suggesting that masks are not only useful but necessary. Ah well – none of us is perfect.
He also observes that the provision of adequate reserve capacity might lead to inefficiency and laziness. It occurs to me that if efficient armies (which do exist, here and there) manage to maintain strategic reserves without altogether lapsing into otiose hebetude and pandiculation, hospitals should be able to.
If anyone is interested in following up the topic of “strategic reserves” in more depths, I very strongly recommend a book that is devoted to this topic:
“Slack: Getting Past Burnout, Busywork, and the Myth of Total Efficiency” by Tom DeMarco.
DeMarco’s very important warning is that the pursuit of total efficiency risks disaster when “black swan events”, or even normal variations, arise.
“Let us be clear, the 50% adjustments are no more than guesses. There are estimates of the extent of over attribution of covid as the cause of death…”
In other words, they are models on which scenarios of future developments might be based. Like Professor Ferguson’s models, only far less extravagant.
Maybe Dr No should see if the government is prepared to bung him a few million for them. (But if I were he I shouldn’t hold my breath).
The powers that be gambled on vaccines saving the day and saving the NHS. That was it, that was the winter plan. Vaccines and some more vaccines. And tests, lots of tests.
There is no plan B to prevent the non-Covid deaths.
Thank you all for your valuable comments. Tom – ” lapsing into otiose hebetude and pandiculation” – you have conclusively managed to out-wordsmith the wordsmith in Dr No!
Dr No left out the what is causing the excess deaths question, deliberately leaving it hanging in the air. Of dearieme’s four suggestions, (ii), delayed diagnosis and treatment, seems on balance likely to have contributed the most, and in the fullness of time, the breakdown of mortality by cause should at the very least give us clues as to whether this is the case, though firm conclusions may be difficult, because the numbers in each category will be small, even if the total number is significant, certain in human cost terms, but also on occasions in statistical terms (see below). Cause (iii), mental health effects, is very plausible but even harder to investigate, as is cause (iv), economic effects. Cause (i), adverse vaccine effects, direct or indirect, likewise is tricky to investigate given currently available data. Nonetheless, it is notable that the sustained unexpected summer excess starts during a time of high vaccination activity. Peter’s FOI request will hopefully bear fruit on this one.
Helen – the powers that be don’t think there are excess deaths, despite the evidence on ONS’s weekly deaths pages (where the data for the above charts came from). The PHE/UKHSE continue to intone “In week XX 2021, no statistically significant excess all-cause mortality by week of death was observed overall in England through the EuroMOMO algorithm” despite the twin tits-up peaks clearly visible in the chart on the same page. Perhaps the numerologically tweaked EuroMOMO algorithm, as well as scrambling the reasoning centres of the brain, also causes cortical blindness. Here is UKHSA’s latest EuroNONO (sic) plot:
And while we are at it, here is ONS’s latest weekly deaths plot for England (Wales is similar, but more jagged, because of smaller numbers):
Both clearly show something is going on…
While writing this post, Dr No did attempt a very crude assessment of whether the individual weekly excesses were statistically significant, by taking an average of the standard deviation (SD) of the number of deaths in each week over the last ten years, and then setting the ‘normal range’ as 1.96 times the SD. It’s a very crude estimate because it takes no account of seasonality – it’s just the average of all weeks over the last ten years – and using it assumes a normal (classic bell shaped) distribution, but with those caveats in mind, weeks 32 and weeks 36 to 38 did have statistically significant excess deaths. The other thing is the excess is consistent over time, if in your mind’s eye you smooth out the BH trough/peak. If the variability was random, it should cut both ways (as in 2020). In 2021 it all went one way…
Dr No, I cannot tell a lie – “otiose hebetude and pandiculation” is not mine. I found it in the American novelist Edgar Pangborn’s novel “A Mirror for Observers” about 50 years ago, and it has stuck in my mind ever since. From time to time I trot it out, as a woman might seize a chance to show off her one and only designer frock.
When reading dearieme’s comment, my immediate reaction was that all four causes look very plausible, although – as Dr No says – it would be hard to say which preponderates. (Oh dear, I seem to have caught the “swallowed a dictionary” bug…)
But if the gubmint don’t think there have been excess deaths… moreover, with everything they have been doing to cause excess deaths…
A few days after every time in the last few months when I’ve mingled indoors with the jab-jabbed, I’ve had a ‘cold’. Not quite the same as a normal cold, but the symptoms each time have been similar.
Could this be an effect of the leaky ‘vaccines’ shedding?
Dearieme, I think you’ve hit the nail on the head with ii and iii; iv will come later. Eventually in the fullness of time we may be able to quantify i, but it may be hard to spot and I expect it will be obscured by the massive collateral damage of all the other stuff, the fear and the isolation and 2 years of NPIs ruinous to public health.
After a decade of UK austerity with underfunding and piecemeal marketisation and privatisation of health and social care and a consequent workforce crisis leading to unsafe staffing levels, we were already seeing reduced bed capacity in hospitals, reduced ambulance response times and delayed hospital discharges. Combine this with an ageing, sedentary, obese population with chronic multi-morbidity and poly-pharmacy and throw in a generous dose of social fragmentation, isolation, loneliness, alcohol and drug dependence and we had a Perfect Storm.
Every winter since I qualified as a GP has seen ambulances backed up outside hospitals, bed crises and cancelled elective surgeries. Increasingly we were seeing this out of season.
I don’t know if it is possible to stop the aerosol spread of a virus in inpatient settings with the Covid infection-control strategies and rituals implemented in the first wave, and little modified since. I do know that increasing social distancing leads to fewer beds, time-consuming infection control and deep cleaning protocols slows things down; controlling entry to hospitals by locking doors and screening all admissions leads to ambulances backing up; requiring a negative PCR 3 days prior to discharge to a care setting or step-down hospital leads to delayed discharges, and reduces available beds; asymptomatic testing of staff, track & trace ping-demic and caution over all colds and flu-like illness leads to prolonged staff absences through quarantining, which further reduces safe staffing levels, appointments and available beds, increases workforce stress and staff sickness; political scapegoating of care home staff over the decisions made in the first wave, the stress and lack of support for carers and threats of mandatory vaccination leads to fewer available care home beds and fewer care packages which leads to delayed discharges and fewer available hospital beds, which leads to slower ambulance response times as ambulances have to travel further when hospitals close to admissions; fear of being responsible or blamed for a vulnerable person acquiring Covid in a health or social care setting means that even in the face of universal vaccination of the vulnerable, these protocols are unlikely to significantly change unless and until there is an honest appraisal of risks versus benefits of all these strategies. Is it controlling Covid or is it the illusion of control at the ‘frontline’? I’ve no doubt people will die as a consequence.
It is scary to see hospitals on Black Alert so early in the season. No wonder there is a call to action from those on the ‘frontline’; it’s like watching a slow car crash. We could take a massive leap of faith and do a Scandinavia, just stop doing much of this ritualistic stuff, that we never did before. Our system had no slack to allow for it – we could have zero Covid and we still wouldn’t cope with a regular winter season with the New Normal protocols. Or we could trigger Plan B or C or whatever iteration we choose of what we have done before, plus vaccine passports and bullying the small proportion of unvaccinated staff into mandatory vaccination with non-sterilising vaccines. Mandatory masks never stopped in Scotland and yet here we are, just the same.
The thing is, those of us in the ‘rear-guard’ see the consequences of two years of the other stuff. Delayed presentations of all sorts of serious illness, a lot of it through fear of Covid (media and govt did and doing a sterling job there), but also real and perceived barriers in access to care and because they were told to ‘stay home, protect the NHS, save lives’; people so terrified of hospitals (of Covid but also of having no visitors and dying alone) that they take their chances at home, leading to worse outcomes and death; fear, social isolation, loneliness, lack of exercise leading to depression, anxiety, frailty, de-conditioning, falls, alcohol dependence, cognitive decline, delirium, obesity, diabetes complications, self harm, family stress, eating disorders in children, domestic violence, child abuse; immunity debt with more severe non-Covid viral infections, delayed elective surgeries and lack of exercise increasing chronic pain; increased prescribing of opioids, antidepressants, gabapentoids, NSAIDs, antipsychotics….increased iatrogenic illness, falls, fractures; fewer face to face medication reviews, missed cues, missed opportunistic diagnoses, late diagnoses…. increased non-Covid deaths.
If, after all this, there are no excess non-Covid deaths, I’ll eat my mask.
It starts with an error in thinking, which is further exasperated by ideology.
At the heart of it is an error in thinking around the money system. The error is in believing that governments must tax to spend, or they must borrow money.
It may have been partially true when the USA was on the gold standard and the UK pound was linked to the USA dollar, but that was dropped early in the 1970s.
The problem is that 99.999% of the population is unlikely to understand how the money system really works, and it’s easy to go with what seems obvious and is the current narrative, IE, tax or borrow.
But it’s this thinking which drives efficiencies and destroys resilience, especially when coupled with neoliberalism.
Hospital beds have halved since the end of the 1980’s. According to this report
“The total number of NHS hospital beds in England, including general and acute, mental illness, learning disability, maternity and day-only beds, has more than halved over the past 30 years, from around 299,000 in 1987/88 to 141,000 in 2018/9, while the number of patients treated has increased significantly”.
Efficiency sounds great until one see’s the true nature that it destroys resilience
You will see efficiencies like this everywhere, but at what real cost to our wellbeing? Another example is our reserves of gas. The UK government recently cancelled our gas storage facilities, so we end up with a couple of weeks in reserve, Germany has several month’s gas storage.
Back to the NHS and beds…
We have amongst the highest occupancy rates and the lowest number of beds per 100,000 IE greater efficiency. I think we are around 2.54 beds per 100,000, France is 5.98, Germany is 8.0
The end result is of course less real efficiency as ambulances get backed up, people are left waiting and so on.
Unfortunately this won’t be solved by changing government. I think it was new labour who decided to ramp up PFI, another great misleading cock-up which we or the NHS and our Schools will be paying massively over the odds for decades to come.
The seat of all this is a highly politicised money system, which is kept obfuscated. The narrative won’t change until people understand it.
Tom – you are forgiven. No wordsmith has ever totally managed to avoid standing on the shoulders of the giants who went before. The phrase is so perfect Dr No was tempted to work it into his latest post (Macavity, about to be published very shortly) but by an effort of will managed to avoid doing so.
Ed P – Dr No hasn’t really looked into ‘leaky’ vaccines yet, so not easy to give an answer.
Helen – another of your brave, and excellent, essays. And good to read someone who is not afraid of long sentences. You are in good company. “It was the best of times, it was the worst of times…”